Note: There is a poll embedded within this post, please visit the site to participate in this post’s poll.
If you’ve heard of billionaire Bryan Johnson, you’ve likely encountered the phrase “bio age testing.”
Johnson, the subject of the Netflix documentary Don’t Die, says he’s on a quest to achieve the lowest possible “biological age” (also known as bio age).
He reportedly spends millions each year on anti-aging treatments—dozens of daily supplements, weekly acid peels for his skin, injections to boost collagen production, hyperbaric oxygen therapy, and plasma infusions extracted from his 17-year-old son’s body.
To determine what’s working, Johnson has undergone numerous tests to assess his bio age. Johnson says these tests show his age is now 5.1 years younger than when he embarked on his anti-aging quest.
Apparently, he’s aging in reverse.
Granted, not everyone’s buying it. A New York Times exposé, for example, claims Johnson’s biological age, in reality, has increased by 10 years.1
Still, Johnson’s “don’t die” crusade is gaining traction.
Bio age tests are a frequent topic on popular podcasts by Peter Attia, Joe Rogan, and Andrew Huberman. Google “bio age testing” and you’ll see dozens of ads for mail-order blood or urine testing kits that claim to reveal your biological age, pace of aging, and more. With prices tumbling into affordability, it’s natural to wonder…
Should you or your client sign up for bio age testing?
If so, which test is best? Just as importantly, what should you do with the information?
In this story, you’ll learn:
- Five FREE ways to assess your overall health and pace of aging—from the comfort of your own home
- Doctor-approved bio age tests you may have already done without realizing it
- The research behind commercial bio age tests, and whether they’re worth your money
- The two biggest mistakes people make when chasing health and longevity
What is your bio age?
Your biological age (bio age) refers to how your cells function. It’s not necessarily the same as your chronological age, which refers to the number of candles on your birthday cake.
For example, let’s say Chang, a 50-year-old man, works at a desk, spends his free time in front of the TV, lives in the most polluted city in the world, eats a candy bar for lunch, and smokes. On the other hand, Jabari, a different 50-year-old man, hits the gym several times a week, lives in the mountains, doesn’t smoke, relishes his five servings of veggies a day, meditates, and spends most evenings in his garden.
Genetics aside, you’d be wise to wager that Jabari’s bio age is younger than Chang’s.
How do these tests measure bio age?
Bio age testing kits measure one or more biological markers of aging, also known as biomarkers.
For example, some tests focus on the size of your telomeres, the protective caps at the ends of chromosomes. Others measure DNA methylation, a physiological process that chemically alters DNA.
Once a company isolates and measures these markers from your blood or urine, it plugs the bio data into a formula that calculates your bio age.
However, if you see a doctor with any regularity, you’re likely already tracking some biomarkers of aging. For example, biomarkers such as blood pressure, cholesterol levels, and blood glucose can help predict your risk of future cardiovascular disease, a leading cause of premature death.
What’s the point of biomarker testing?
Biomarker testing can help you monitor your wellness proactively rather than waiting for disease symptoms to appear.
For some, it also serves as a motivator. If you learn you have the bones of someone 20 years older, this may give you the nudge you need to start strength training consistently.
In addition, biomarkers provide objective data, allowing you to track and evaluate various health-related actions quantitatively. By monitoring your blood pressure, you might learn that consistent exercise helps, but your late-afternoon energy drink does the opposite.
5 FREE biomarker tests
You don’t have to be a billionaire (or even a millionaire) to track biomarkers of aging.
In this section, we’ll cover several massively underappreciated, scientifically validated tests you can use to gain insight into your bio age—for FREE.
Before scientists developed high-tech blood-based bio age tests, researchers used these free tests to calculate the pace of aging in the people they studied.
FREE biomarker test #1: Get off the floor
People who are fitter and stronger tend to live longer.2
That’s because muscles do more than just move us around. They also secrete anti-inflammatory substances, help to regulate blood sugar, slow cellular aging, protect the lining of the arteries, and more. All this helps reduce the risk of age-related diseases, such as type 2 diabetes, high blood pressure, and heart disease, a phenomenon we explore in our article, The New Science of Muscle.
Related to strength, your ability to balance is also key. If you’re middle-aged or older and can’t stand on one foot for at least 10 seconds, your risk of dying in the next seven years is double that of someone who can stand for longer, according to a study of 1,700 people.3
The Sitting-Rising Test (SRT) is one way to assess both strength and balance at the same time.
People with low scores on this test have a higher risk of dying from cardiovascular disease, according to a 12-year study of 4,200 adults between the ages of 46 and 75.4
 How to measure it
How to measure it
Lower yourself to the floor with your legs in a crisscross position. Then, with your legs in the same position, stand back up. As you stand, notice if you must use a part of your body—hand, shin, knee—as leverage.
To score yourself, start with 10 points. Then, for each body part you used to stand, deduct a point. Subtract a half point if you became unsteady or lost your balance.
Keep in mind that this (and other tests) serve as a proxy for your fitness. A low score indicates that your balance and coordination, muscle strength and power, and mobility may all require some attention.
FREE biomarker test #2: Squeeze a ball
Like the SRT test, your grip strength provides insight into your overall fitness. If the muscles in your hands are weak, the muscles throughout your body are more likely to be weak, too.
Poor grip strength can also predict future muscle weakness. In one study, people with a weak grip were more likely to walk slowly and be unable to rise from a chair, complete rigorous housework, or climb a flight of steps 25 years later.5
Low grip strength has also been associated with:6
- Low bone mineral density
- Increased risk of falls
- Poor nutritional status
- Depression
- Poor sleep, cognitive function, and/or quality of life
- Increased risk of heart disease, cancer, and premature mortality
According to one study, grip strength was a better indicator of longevity (or lack thereof) than blood pressure.7
How to measure it
Grab a standard tennis ball, and squeeze as hard as you can, for as long as you can.
If you can manage 15 to 30 seconds before your grip fatigues, you’re doing fine. Ninety seconds puts you well above average—anything over 90 ranks you solidly in the upper-third percentile.
If you’re below 15, keep in mind that this test is also just one indicator of your overall strength. (And squeezing balls to improve grip strength without training the rest of your body is unlikely to make significant improvements in your overall health and fitness.)
A hand-held dynamometer—available for use at most occupational therapists’ and some gyms—can also test grip strength. (If you’re willing to shell out some cash, you can buy your own for somewhere between $100 and $500.)
FREE biomarker test #3: Stand on one foot
An ability to balance on one foot for an extended period can help reduce your risk of falls, one of the leading causes of injury-related death among older adults.
In addition, many different bodily systems—the eyes, inner ear, skeletal muscles, and brain—must work together to help you stay upright.
Conditions like diabetes, heart disease, and cancer can all affect balance. As a result, an inability to stand on one foot can serve as a warning sign for eroding health and fitness.8
How to measure it
Stand near a wall or chair for safety. Keep your eyes open and hands on your hips. Then, lift your dominant leg and start timing yourself. Once you put your foot down, stop the clock. Repeat the test with your non-dominant leg.
Once you have your times, compare them to the following averages, from a study out of Duke University, to see how you did compared to your age-matched peers.9
| Age | Seconds on one leg (males) | Seconds on one leg (females) |
|---|---|---|
| 30-39 | 59 | 56 |
| 40-49 | 56 | 55 |
| 50-59 | 42 | 48 |
| 60-69 | 40 | 38 |
| 70-79 | 27 | 25 |
| 80+ | 13 | 11 |
FREE biomarker test #4: How you feel
Sometimes you know why you’re tired, such as the morning after binge-watching the last few episodes of a thriller. Once you catch up on your sleep, the weariness lifts.
That’s not the same thing as fatigue, which describes persistent exhaustion that worsens over time and interferes with life. In addition to feeling physically tired, someone who’s fatigued feels mentally dull and emotionally exhausted.
Think of fatigue as an early sign that something’s off, especially if you don’t know the cause.
Let’s say you’ve already ruled out the usual suspects like too much caffeine, dehydration, too much alcohol, medication side effects, chronic stress, or too much or too little exercise. What’s left is likely a sleep disorder or a developing health problem such as anemia, obesity, depression, cancer, or diabetes, to name a few.
If you’re 60 or older, fatiguability—or how worn out you feel after an activity—can also predict longevity.
According to research out of the University of Pittsburgh Medical Center, the higher someone scores in fatiguability, the higher their risk of death in the future.10 Other research has linked high fatiguability with declines in gait speed, walking ability, and other tests of fitness.11
How to measure it
To measure fatigability, use a tool called the Pittsburgh Fatigability Scale. Using a 0 (no fatigue) to 5 (extreme fatigue) scale, rate how fatigued you think you would feel after completing the following activities:
| Activity | Duration | Score (0 to 5) |
|---|---|---|
| Leisurely walking | 30 minutes | |
| Brisk or fast walking | 1 hour | |
| Light household activity | 1 hour | |
| Heavy gardening or yard work | 1 hour | |
| Watching television | 2 hours | |
| Sitting quietly | 1 hour | |
| Moderate-to-high intensity strength training | 30 minutes | |
| Participating in a social activity | 1 hour | |
| Hosting a social event for 60 minutes | 1 hour | |
| High intensity activity | 30 minutes | |
| Add all scores: | ||
If you score less than 15, you’re doing well. Scores between 15 and 24 are a warning sign. Anything 25 and above is regarded as severe, and worth mentioning to your healthcare professional.12
FREE biomarker test #5: Body composition
Despite popular belief, both too little and too much body fat can influence health for the worse, as we explore in our infographic, Is body fat good or bad for you?
| Too much fat raises the risk for: | Too little muscle raises risk for: |
|---|---|
| Heart disease | Heart disease |
| High blood pressure | High blood pressure |
| Cancer | Cancer |
| Fatty liver disease | Stroke |
| Insulin resistance | Insulin resistance |
| Type 2 diabetes | Faster cellular aging |
| Inflammation | Inflammation |
| Joint distress | Depression and anxiety |
| Sleep apnea | Falls and loss of balance |
Your muscle mass also plays a role, which is why someone’s body composition matters more than their weight.
The gold standard methods that estimate body composition—underwater weighing, air displacement (Bod Pod), and dual-energy X-ray absorptiometry (DEXA)—certainly aren’t free.
However, a recent study determined that a good old-fashioned (and cheap) tape measure can provide a comparably accurate estimate of body composition.13
How to measure it
To use a tape measure to keep track of your body fat percentage, measure:
- The widest part of your neck
- The narrowest part of your waist (For some people, this will be at the navel. For others, it might be slightly above the navel)
- The widest part of your hips
Ensure the tape is snug but not so tight that it cuts into the skin. Once you have your measurements, plug those numbers—along with your age, sex, height, and weight—into our FREE Body Fat Calculator, which will take it from there.
Doctor-approved biomarker tests
Depending on where you live in the world, the following tests may not be free. However, as part of routine preventative care, your insurance might cover them.
Doctor-approved test #1: Blood panel
If your primary care doctor recommends yearly blood work, it’s for good reason.
By keeping tabs on several blood markers, you can see if your health is trending toward type 2 diabetes or heart disease, both leading causes of premature mortality.
Many blood markers can also be influenced relatively quickly (within 6 to 12 weeks) through lifestyle changes, supplement protocols, or medications. This makes them practical tools for monitoring whether various lifestyle or medical modifications are working.
How to measure it
If you’re not already doing so, consider having the following blood markers tested annually. Then, talk to your health care professional about what your numbers mean. They might use the following numbers, along with your blood pressure, to calculate a cardiovascular disease risk score.
| Blood marker | Optimal range |
|---|---|
| Total cholesterol | < 200 mg/dL* |
| LDL | < 100 mg/dL for those without heart disease < 70 mg/dL for those with a history of heart attack or stroke |
| HDL | > 60 mg/dL |
| Triglycerides | < 150 mg/dL |
| Alipoprotein B (Apo B) | < 133 mg/dL (males) < 117 mg/dL (females) |
| Lipoprotein (a) | < 30 mg/dL |
| C-reactive protein | < 2.0 mg/L** |
| Fasting glucose | < 100 mg/dL |
| Hemoglobin A1C | < 5.7% |
*Milligrams per deciliter of blood
**Milligrams per liter
Doctor-approved test #2: Bone density
When researchers study healthy super-agers aged 90 and older, strong bones are one of their defining features.14
That may be because, like muscles, bones are live organs that secrete substances that may be beneficial to overall health and longevity.15
For example, bones secrete osteocalcin, a hormone that plays a role in bone remodeling. When osteocalcin circulates in the body, it’s thought to play a role in everything from helping muscles to produce ATP to regulating brain neurotransmitters.
Because of these varied roles, it’s thought that, as bones wear away, osteocalcin levels drop, contributing to many age-related health problems, including diabetes, low muscle mass, and cognitive issues.16 17 (At least, that’s the theory. Most of this research has been done on mice.)
Osteocalcin aside, loss of bone density can, of course, lead to fractures, which can increase your risk of death for up to 10 years after a break.18
It’s especially important to keep tabs on bone health if you’re in any of these high-risk categories:
- You’re female and went through menopause before age 45.
- You’ve been sedentary most of your adult life.
- You take medications such as diuretics or stomach-acid blockers, which are linked with an increased risk of osteoporosis.
- You have a history of nicotine use or excessive alcohol consumption.
- You have a medical condition, such as diabetes or thyroid disease, that raises your risk.
- You have a family history of osteoporosis.
How to measure it
Dual-energy X-ray absorptiometry (DEXA) scans are a type of X-ray that measures the amount of bone mineral content packed into a square centimeter of bone.
Insurance often won’t cover these scans for people younger than 65 unless there’s a documented risk of developing osteoporosis. Out of pocket, the average cost is about $300.
When you receive your DEXA results, you’ll see a T-score that represents how your bone density compares to the average bone density of a young adult with peak bone mass. A T-score of +1.0 to -1.0 means you have normal bone mineral density for someone your age. Anything below -1.0 means you might have osteopenia (low bone mineral density) or osteoporosis (porous bones that are prone to fracture).
Commercial bio age tests
If you have some money to burn, you can learn an awful lot about your body.
Here, you’ll find a quick run-down on some of the more high-tech tests you can get and what they can tell you.
However, before we get into the details, we want to point out a few caveats:
Biological age can vary over time, and by organ. Someone may go through a period of accelerated aging—saying, during a period of intense stress—then their rate of aging may slow as they focus more on recovery. Additionally, organs can age at different rates. For example, someone with heart disease may have a relatively older heart than their kidneys. (Not all tests measure individual organ age, but it’s becoming more common.)
Commercial tests won’t always accurately reflect the changes you’re making. Until more research supports the reliability of these tests, evaluate your behaviors over isolated test results. If you’re eating more fruits and veggies, exercising more consistently, managing stress, and otherwise slaying the healthy lifestyle department, don’t sweat your results. Focus on doing the things we know improve health.
If a company pairs your test results with a hard sell for a proprietary and expensive supplement protocol, be wary. It’s better to share and discuss your results with a trusted health professional than take health advice from a profit-seeking stranger over the internet.
Commercial test #1: DNA methylation
DNA methylation is a biological process that chemically alters DNA. Because the rate of methylation accelerates with aging, it can be used to estimate someone’s biological age and life expectancy, finds research.19 20 21
The Horvath Clock and DunedinPACE both measure specific biomarkers that can be used to better understand someone’s methylation rate. Scientists developed these tests to help other scientists study how various lifestyle factors, environmental exposures, and medicines affect aging. They didn’t develop the tests as a way for the average person to pinpoint their biological age. (Which hasn’t stopped companies from selling DNA methylation testing kits to the public.) They cost about $300.
If you decide to get one of these tests, keep in mind your results won’t give you a complete picture of your health and longevity. Aging typically occurs at varying rates throughout the body. Your liver might age faster than your heart or brain, for example. So if you measure DNA methylation in your blood, that’s all you know about. Put another way, a DNA methylation test isn’t a substitute for your annual wellness checkup or blood work.
Commercial test #2: Telomere analysis
Telomeres—the protective caps on the ends of chromosomes—wear away with age. The length of a telomere can predict how many times a specific cell can divide before dying.
Abnormally short telomeres are associated with several genetic diseases. For this reason, when physicians suspect someone might have inherited a genetic disease, they’ll order a specific type of telomere test—the flow-FISH test—to measure the telomere length in all the cells in a blood sample.22 23
It’s more debatable whether telomere tests can predict aging in healthy people.
Just as importantly, the telomere test marketed to the public, known as the qPCR telomere test, isn’t used in research or medicine. These $100 tests are fine if you’re merely curious—just don’t base health and fitness decisions on your results.
Commercial test #3: VO2 Max
For years, only elite athletes cared about VO2 max, which describes the maximum amount of oxygen that your body can use during exercise.
More recently, however, some experts have suggested that VO2 max can serve as a measure for athletes and non-athletes alike to track the rate at which their bodies are aging.
People with high VO2 max tend not only to be more physically fit but also less likely to develop heart disease, diabetes, cancer, or stroke.24 25 26 27
In an observational study that followed the health outcomes of 5,107 Danish men over 46 years, men with above-average V02 max during middle age lived an average of five years longer than men with below-average V02 max. Each unit increase in VO2 max was associated with a 45-day increase in longevity. The researchers suggested VO2 max may more accurately predict all-cause mortality than high cholesterol, obesity, high blood pressure, and insulin resistance.28
You might think of V02 max as a canary and your aging body as a coal mine.
As you age, your chest wall becomes more rigid, the muscles that surround the lungs weaker, and the oxygen-carrying blood vessels calcified and less elastic. The heart also squeezes with less force, max heart rate drops, muscle mass and strength decline, the mitochondria in cells and muscles lose their effectiveness, among other differences.
In addition to raising your risk for many different diseases, these changes can also affect VO2 max, which tends to decline 10 percent per decade starting around age 30.29 30
In the past, the only way to reliably measure VO2 max was in a fitness lab.
You would wear a metabolic mask and a heart monitor while you ran or cycled to exhaustion. The mask collected your expired carbon dioxide and monitored how much oxygen you sucked into your lungs. This lab-based testing is still the most accurate way to measure V02 max as well as other key fitness metrics such as:
- Max heart rate, or the highest number of times your heart can beat per minute during exercise
- Ventilatory threshold 1, or the point during exercise when the body switches from mainly using fat for fuel to using a combination of fat and glucose or glycogen (stored glucose) for fuel.
- Ventilatory threshold 2, or the point where your body moves away from aerobic metabolism (which uses oxygen) to anaerobic metabolism (which doesn’t use oxygen).
- Tidal volume is the amount of air inhaled or exhaled during each breath
Depending on where you live, you might be able to get your VO2 max tested for around $150.
However, if you don’t have access to a VO2 max clinic, three somewhat less accurate options exist.
The 1-mile walk test
Wear a heart rate monitor as you walk one mile on a flat surface, such as a treadmill or running track. As soon as you complete the mile, record your heart rate and walk time. Then, plug it into the following formula to calculate your VO2 max:
132.853 — (0.0769 × Weight) — (0.3877 × Age) + (6.315 × Sex) — (3.2649 × Time) — (0.1565 × Heart rate)
If that feels like too much math, you can also use a free online tool.
The smartwatch test
Many smartwatches will estimate your VO2 Max for you based on information the watch gathers from your workouts, sex, and age. Compared to in-office testing, smart watches can over- or underestimate V02 max, especially in people who are very out of shape or extremely fit.31
Because of this, you don’t necessarily want to use your smart watch measurement to determine your current state of health. However, it can help you to see trends. For example, does your VO2 estimate drop after a few weeks of skipping your usual spin class? If so, that’s good information to have.
The PR test
Fitness performance correlates with longevity. If you’re getting faster at running a certain distance or can go a longer distance than before, you’re getting fitter and increasing your chances of living a long, healthy life.
One way to test this: the 12-minute run test, also known as the Cooper test. (This is a validated way to estimate VO2 max—and shows about a 90 percent correlation with lab-based measurements.)
Here’s how it works:
Run as fast as you can on a flat surface, such as a treadmill set at a 1 percent incline or running track, for 12 minutes. After 12 minutes, record your distance. Then, plug it into one of the following formulas to calculate your VO2 max.
| Distance in Miles | Distance in Kilometers | |
|---|---|---|
| VO2 Max = | (35.97 x distance in miles) – 11.29 | (22.351 x distance in kilometers) – 11.288 |
In lieu of doing math, you can also use a free online calculator.
How to change your biological age
Try to think of the information you gather about your body as just that—information.
It’s not a moral judgment of who you are as a person.
Just as importantly, it’s not a permanent situation.
- If you’re weaker than other people your age, you can grow stronger.
- If your cholesterol or blood glucose levels are high, you can take steps to lower them.
- If your body is aging faster than your birthdays, consider exploring key lifestyle changes that may help turn the situation around.
You have options. However, most people make two big mistakes when it comes to longevity-related lifestyle changes.
Mistake #1: Ignoring evergreen, big-impact strategies
It’s the simple, boring, “I’ve heard this a million times before” health practices that, when done consistently, add up to a long, healthy life.
We’re talking about things like…
- Eating more minimally processed foods and fewer ultra-processed foods
- Consuming more brightly colored fruits and veggies
- Moving your body regularly
- Getting enough rest and sleep
- Enjoying community, time in nature, and other activities that make life meaningful
- Keeping alcohol intake moderate
- Not using tobacco
- Wearing sunscreen
- Flossing
And that’s just a partial list.
According to thousands of studies, people who practice these and other high-impact strategies not only live longer, but also live better. They’re stronger, happier, and less likely to spend their later years disabled or in pain.
(If you’d like to see where you stand when it comes to big impact health and longevity strategies, check out our FREE Longevity Assessment.)
However, when it comes to health, fitness, and longevity, many people pursue options with minimal impact (at best). They reach for the latest, trendy supplement rather than taking steps to quit smoking, as just one example.
Here’s the thing: Big rock strategies require changes in behavior. If daily physical activity were as easy as popping a pill, walkers and cyclists would clog up the streets in your neighborhood.
(It’s precisely this reason why so many people need the support of a certified health coach who has undergone training in the science of behavior change.)
Mistake #2: Not turning data into action
The data gathered from biomarker aging tests can give you a sense of control.
However…
Data, in isolation, doesn’t lead to a longer life.
Gathering data without changing your behavior is like checking your reflection in the mirror, seeing spinach wedged between your incisors, and leaving it there.
You need to remove the spinach for the mirror check to be worthwhile.
Biomarker testing is the same.
If you don’t use your bio data to inform behavior change, you’re wasting your money and time.
Consider your biomarker data as a baseline or starting point.
Then, use it to assess whether various lifestyle changes or medical interventions are moving you closer to your goal of living a longer, healthier life.
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
1. Grind K. How Bryan Johnson, Who Wants to Live Forever, Sought Control via Confidentiality Agreements. The New York Times [Internet]. 2025 Mar 21 [cited 2025 Jul 15]; Available from: https://www.nytimes.com/2025/03/21/technology/bryan-johnson-blueprint-confidentiality-agreements.html
2. Strasser B, Volaklis K, Fuchs D, Burtscher M. Role of dietary protein and muscular fitness on longevity and aging. Aging Dis. 2018 Feb 1;9(1):119–32.
3. Araujo CG, de Souza E Silva CG, Laukkanen JA, Fiatarone Singh M, Kunutsor SK, Myers J, et al. Successful 10-second one-legged stance performance predicts survival in middle-aged and older individuals. Br J Sports Med. 2022 Sep 1;56(17):975–80.
4. Araújo CGS, de Souza e Silva CG, Myers J, Laukkanen JA, Ramos PS, Ricardo DR. Sitting–rising test scores predict natural and cardiovascular causes of deaths in middle-aged and older men and women. Eur J Prev Cardiol. 2025 Jun 18;zwaf325.
5. Dodds RM, Kuh D, Sayer AA, Cooper R. Can measures of physical performance in mid-life improve the clinical prediction of disability in early old age? Findings from a British birth cohort study. Exp Gerontol. 2018 Sep;110:118–24.
6. Bohannon RW. Grip strength: An indispensable biomarker for older adults. Clin Interv Aging. 2019 Oct 1;14:1681–91.
7. Leong DP, Teo KK, Rangarajan S, Lopez-Jaramillo P, Avezum A Jr, Orlandini A, et al. Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet. 2015 Jul 18;386(9990):266–73.
8. Rezaei A, Bhat SG, Cheng C-H, Pignolo RJ, Lu L, Kaufman KR. Age-related changes in gait, balance, and strength parameters: A cross-sectional study. PLoS One. 2024 Oct 23;19(10):e0310764.
9. Hall KS, Cohen HJ, Pieper CF, Fillenbaum GG, Kraus WE, Huffman KM, et al. Physical performance across the adult life span: Correlates with age and physical activity. J Gerontol A Biol Sci Med Sci. 2017 Apr 1;72(4):572–8.
10. Glynn NW, Gmelin T, Renner SW, Qiao YS, Boudreau RM, Feitosa MF, et al. Perceived physical fatigability predicts all-cause mortality in older adults. J Gerontol A Biol Sci Med Sci. 2022 Apr 1;77(4):837–41.
11. Simonsick EM, Schrack JA, Santanasto AJ, Studenski SA, Ferrucci L, Glynn NW. Pittsburgh Fatigability Scale: One-page predictor of mobility decline in mobility-intact older adults. J Am Geriatr Soc. 2018 Nov 1;66(11):2092–6.
12. Vercelli S, Zampogna E, Negrini F, Pietraroia C, D’Antona G, Papa S, et al. Cross-cultural translation, validation, and responsiveness of the Pittsburgh Fatigability Scale – Italian version (PFS-I) in a mixed-sample of older adults. BMC Geriatr. 2024 Dec 19;24(1):1016.
13. Combest TM, Khan J, Tufano JJ, Lane M, Watson NL, Altom KR, et al. Comparison of four body composition methods: Circumference measurements, eight-point bioelectrical impedance analysis up to 500 and 1000 kHz to dual-energy X-ray absorptiometry to measure body fat percentage. Mil Med [Internet]. 2024 Sep 18 [cited 2025 Jan 11]
14. Dayer SR, Mears SC, Pangle AK, Mendiratta P, Wei JY, Azhar G. Does superior bone health promote a longer lifespan? Geriatr Orthop Surg Rehabil. 2021 Aug 3;12:21514593211036231.
15. Mera P, Laue K, Wei J, Berger JM, Karsenty G. Osteocalcin is necessary and sufficient to maintain muscle mass in older mice. Mol Metab. 2016 Oct 1;5(10):1042–7.
16. Weivoda MM, Chew CK, Monroe DG, Farr JN, Atkinson EJ, Geske JR, et al. Identification of osteoclast-osteoblast coupling factors in humans reveals links between bone and energy metabolism. Nat Commun. 2020 Jan 7;11(1):87.
17. Lee NK, Sowa H, Hinoi E, Ferron M, Ahn JD, Confavreux C, et al. Endocrine regulation of energy metabolism by the skeleton. Cell. 2007 Aug 10;130(3):456–69.
18. Tran T, Bliuc D, Hansen L, Abrahamsen B, van den Bergh J, Eisman JA, et al. Persistence of excess mortality following individual nonhip fractures: A relative survival analysis. J Clin Endocrinol Metab. 2018 Sep 1;103(9):3205–14.
19. Chen BH, Marioni RE, Colicino E, Peters MJ, Ward-Caviness CK, Tsai P-C, et al. DNA methylation-based measures of biological age: meta-analysis predicting time to death. Aging (Albany NY). 2016 Sep 28;8(9):1844–65.
20. Lu AT, Quach A, Wilson JG, Reiner AP, Aviv A, Raj K, et al. DNA methylation GrimAge strongly predicts lifespan and healthspan. Aging (Albany NY). 2019 Jan 21;11(2):303–27.
21. Belsky DW, Caspi A, Corcoran DL, Sugden K, Poulton R, Arseneault L, et al. DunedinPACE, a DNA methylation biomarker of the pace of aging. Elife. 2022 Jan 14;11:e73420
22. Alder JK, Hanumanthu VS, Strong MA, DeZern AE, Stanley SE, Takemoto CM, et al. Diagnostic utility of telomere length testing in a hospital-based setting. Proc Natl Acad Sci U S A. 2018 Mar 6;115(10):E2358–65.
23. Vaiserman A, Krasnienkov D. Telomere length as a marker of biological age: State-of-the-art, open issues, and future perspectives. Front Genet. 2020;11:630186.
24. Imboden MT, Harber MP, Whaley MH, Finch WH, Bishop DL, Kaminsky LA. Cardiorespiratory fitness and mortality in healthy men and women. J Am Coll Cardiol. 2018 Nov 6;72(19):2283–92.
25. Cai L, Gonzales T, Wheeler E, Kerrison ND, Day FR, Langenberg C, et al. Causal associations between cardiorespiratory fitness and type 2 diabetes. Nat Commun. 2023 Jul 3;14(1):3904.
26. Aker A, Saliba W, Bahouth F, Naoum I, Zafrir B. Cardiorespiratory fitness and risk of cardiovascular events and mortality in middle age patients without known cardiovascular disease. J Clin Med. 2023 Nov 9;12(22):7011.
27. Prestgaard E, Mariampillai J, Engeseth K, Erikssen J, Bodegård J, Liestøl K, et al. Change in cardiorespiratory fitness and risk of stroke and death: Long-term follow-up of healthy middle-aged men: Long-term follow-up of healthy middle-aged men. Stroke. 2019 Jan;50(1):155–61.
28. Clausen JSR, Marott JL, Holtermann A, Gyntelberg F, Jensen MT. Midlife cardiorespiratory fitness and the long-term risk of mortality: 46 years of follow-up. J Am Coll Cardiol. 2018 Aug 28;72(9):987–95.
29. Kim C-H, Wheatley CM, Behnia M, Johnson BD. The effect of aging on relationships between lean body mass and VO2max in rowers. PLoS One. 2016 Aug 1;11(8):e0160275.
30. Strasser B, Burtscher M. Survival of the fittest: VO2max, a key predictor of longevity? Front Biosci (Landmark Ed). 2018 Mar 1;23(8):1505–16.
31. Caserman P, Yum S, Göbel S, Reif A, Matura S. Assessing the accuracy of smartwatch-based estimation of maximum oxygen uptake using the Apple Watch Series 7: Validation study. JMIR Biomed Eng. 2024 Jul 31;9(1):e59459.
If you’re a health and fitness pro…
When your clients are stressed and exhausted, everything else becomes a
struggle: going to the gym, choosing healthy foods, and managing cravings.
But with the right tools, you can help your clients overcome
obstacles like chronic stress and poor sleep—leading them toward the
lasting health transformations they’ve always wanted.
PN’s Level 1 Sleep, Stress Management, and Recovery (SSR) Coaching
Certification
will give you these tools. And it’ll give you confidence and credibility as a
specialized coach who can
solve the biggest problems blocking any clients’ progress. (You can
join the SSR Early Access List for our biggest discount + exclusive perks.)
The post Biological age tests: Should you get one? appeared first on Precision Nutrition.
Source: Health1
Many people with IBS would trade 10 to 15 years of life expectancy for an instant cure for their condition.
This is according to the results of a study of nearly 2,000 people with irritable bowel syndrome (IBS).1
In other research, people with IBS said they would take a medicine that carried a one percent risk of sudden death if it would cure their symptoms2—which can include urgent bouts of diarrhea, gas, or persistent constipation.
Some people with IBS experience bouts of abdominal pain they describe as worse than childbirth. These flare-ups can siphon concentration, interrupt sleep, and destroy work productivity.3
As a result, many people with IBS plan their lives around the availability of private, clean bathrooms. Fear of a sudden flare-up leads some to avoid restaurants, get-togethers, even exercising in public.
This pervading worry has a name—gastrointestinal-specific anxiety—and it can affect everything from social relationships to overall well-being. It’s also the main reason people with IBS report worse quality of life than people with other chronic conditions, including heart disease, diabetes, and end-stage kidney disease.4
If you or a client has IBS, there are ways to manage it.
PN Super Coach Sarah Maughan, certified through Monash University—a global leader in understanding the link between food sensitivities and IBS—has witnessed how lifestyle changes can prevent flare-ups, calm GI anxiety, and allow people with IBS to live the lives they want.
“My hope is for everyone with IBS to know they have options, whether that’s turning to a physician for medication and/or a health coach to learn about lifestyle changes and how to put them into action,” says Maughan.
In this article, we’ll hear more from Maughan. You’ll also learn:
- What IBS is, including why it happens and the different ways it can manifest
- What your poo can tell you about the health of your digestive tract
- Five evidence-based lifestyle changes that can improve IBS symptoms
- The best way to determine which foods trigger your or your client’s IBS symptoms (and which foods are usually “safe” to eat)
Plus, if you’re a health coach, you’ll learn how to support clients with IBS while safely staying within your scope of practice.
So, what is IBS?
Sometimes referred to as “spastic colon,” IBS is the most commonly diagnosed digestive disorder in the world, affecting about 14 percent percent of adults.5
Unlike Crohn’s and other inflammatory bowel diseases (IBD), IBS doesn’t alter the architecture of the gut. When healthcare professionals use diagnostic imaging, they find no infections, inflammation, damage to the bowel wall, or other evidence of disease.
Years ago, this lack of visible disease led many healthcare professionals to assume that IBS was purely psychological. More recently, however, this thinking has shifted.
Experts now view IBS as a functional neuro-gastrointestinal disorder.
That means the nerves between the GI tract and the brain don’t function optimally, causing the brain to deliver unnecessary pain signals and interfere with typical bowel function.
What are the symptoms of IBS?
IBS symptoms can come and go, with some people experiencing months or years of relief only to suffer a severe flare-up that can last hours to weeks.
In addition, not everyone with IBS experiences the same set of symptoms, which can make the condition challenging to diagnose.
The below illustration shows the range of IBS symptoms.

What causes IBS?
Researchers are still trying to understand why the gut functions differently in people with IBS. However, they do have a few theories.
According to one hypothesis, the nerve endings in the GI tract may be overly sensitive in people with IBS. This can lead to two different sets of symptoms.
Hypersensitive nerves communicate pain signals to the brain, causing people with IBS to notice digestive processes that other people wouldn’t feel. Tiny gas bubbles may be severely uncomfortable for someone with IBS, for example, but not bother someone without the disorder.
Overreactive nerves can trigger GI muscles to contract with too much force, leading to gas, bloating, and diarrhea. If they underreact, the same muscles don’t contract forcefully enough, which slows the passage of food through the intestine and leads to constipation.
Another theory blames disturbances on the gut microbiome, which helps to explain why some people develop IBS symptoms after first having a severe GI illness like the Norovirus.
How is IBS diagnosed?
If you or your client suspect IBS, see a credentialed health professional.
The symptoms of IBS overlap with several other gastrointestinal diseases and health conditions that can require medication, surgery, or medically-supervised lifestyle changes. These include infections, inflammatory bowel diseases, celiac disease, cancer, and food allergies, among others.
It’s especially important to see a medical professional if you or your client notice any of the following:
- Rapid, unintentional weight loss
- Rectal bleeding, blood in stools, or vomiting blood
- Bouts of diarrhea that disturb sleep
- Diarrhea with fever
- Continuous abdominal pain
- A sudden onset of GI symptoms after age 50
IBS Types
In addition to ruling out other GI conditions, a healthcare professional will also ask detailed questions about you or your client’s symptoms. This information allows them to pinpoint which IBS “type” you or your client might have:
- IBS-D, which means someone predominantly has diarrhea
- IBS-C, which is characterized by constipation
- IBS-M, which means someone has alternating periods of diarrhea and constipation
- IBS-U, which means someone’s symptoms don’t neatly fall into any of the above categories
You or your client’s IBS type will inform what your healthcare professional recommends.
A healthcare provider might suggest a short course of antibiotics and antidiarrheal medicine for IBS-D. On the other hand, for IBS-C, they might recommend a fiber supplement, non-habit-forming laxative, laxative-like medication, or other medicine that reduces the perception of pain and regulates bowel movements.
How to prepare for a medical appointment: Your pre-appointment checklist
In order to get the most out of the visit, you can help your client (or yourself) prepare for a healthcare appointment.
A healthcare professional will likely ask the following questions, so consider the responses beforehand:
- How long have you experienced these symptoms?
- Did anything change around the time your symptoms began? (Stress levels? Dietary habits? Recent travels?)
- Did you recently have food poisoning or gastroenteritis?
- How much fiber do you consume?
- How is your sleep quality? How many hours do you usually sleep at night?
- How often do you exercise?
Another way to prepare for your first appointment?
Well, you might not like it, but it’s a good idea to…
Look at your poo
Consider keeping a poo diary for a couple of weeks before your appointment.
In the diary, track the frequency of bowel movements and other symptoms. Use the Bristol Stool Chart (below) to take note of the quality of your poo. This information can help your healthcare professional assess whether you have IBS and which type.

(To learn more about the clues your poos can hide, read: 6 reasons you should care about your poop health)
How to help IBS: 5 strategies to support bowel health and function
In recent years, the U.S. Food and Drug Administration approved several new prescription medicines for IBS, along with a medical device that stimulates the cranial nerves behind the ear.
In addition, thousands of research papers have looked at the interaction between IBS and various lifestyle habits, with many promising findings.
Here are five evidence-based ways to reduce the symptoms of IBS (and bonus, many of them are great for enhancing overall health too).
IBS relief strategy #1: Add exercise
People with IBS who exercise regularly tend to experience fewer symptoms and flare-ups than people who don’t exercise.
When researchers asked people with IBS to walk moderately for an hour three times a week, study participants experienced significant relief from bloating and abdominal pain within 12 weeks.6
How exercise soothes IBS isn’t fully understood, though.
According to other research, exercise may reduce stress and improve mental health, which, in turn, may help improve communication between the gut and the brain.7 8
Another theory argues that exercise helps encourage the growth of health-promoting gut bacteria, which may help to break down food more efficiently and decrease inflammation.9
IBS relief strategy #2: Work on stress management
Anxiety, stress, and depression all activate stress hormones like norepinephrine (noradrenaline) and cortisol, which can:
- Amplify gut-based pain signals
- Alter the balance of bacteria in the gut (known as the gut microbiome)
- Increase intestinal permeability—potentially allowing harmful substances into the bloodstream10 11 12
Of course, stress doesn’t come with an on/off switch.
Simply telling yourself, “Stop getting so stressed out!” won’t likely help—and may even paradoxically lead to more stress.
That’s why Precision Nutrition-certified coaches like Maughan help clients learn to focus on what’s within their control—such as practicing self-compassion, or experimenting with nervous system regulators like yoga, breathing exercises, and gentle walking.
As the image below illustrates, clients can control how they perceive, respond to, and anticipate stressors—but not always the stressors themselves.
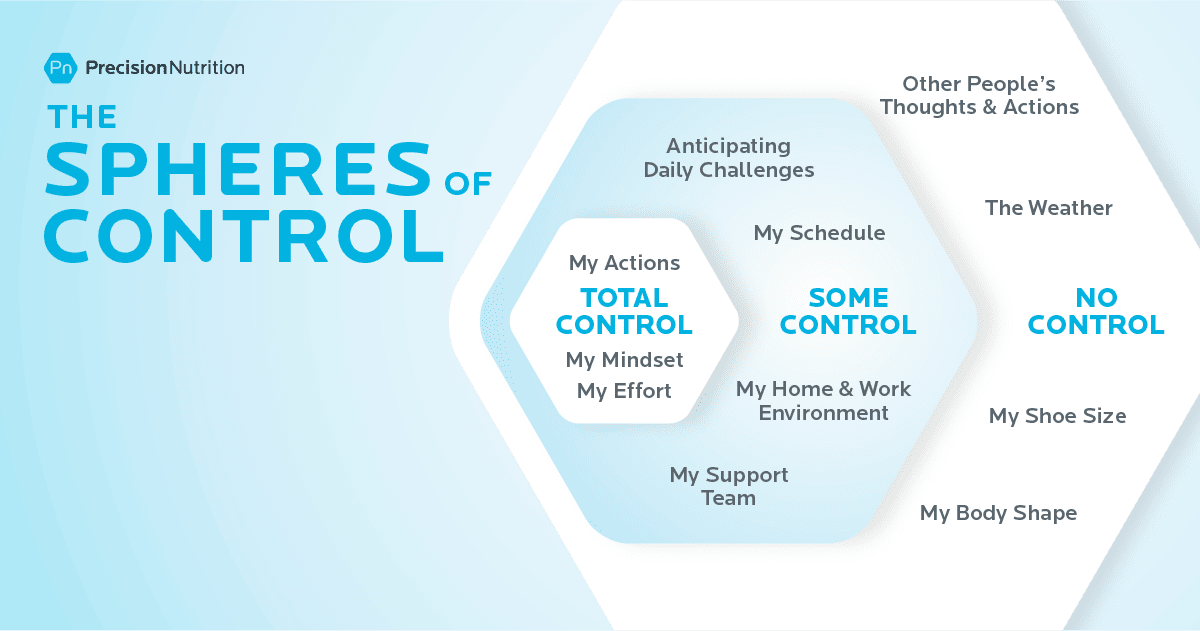
Either way, when clients focus more on what they can control and less on what they can’t, they often feel calmer and more capable.
(If you want to help a client figure out just what’s within their control—and what’s not—try out our free worksheet: Sphere of Control Worksheet)
(Assess your current stress load by taking our free quiz: Do you have a Stress Bod?)
IBS relief strategy #3: Slow your eating pace
PN coaches have long appreciated and advocated slower, more relaxed eating.
Yes, slow eating helps people fill up on fewer calories—but it also tends to help clients reduce or even eliminate GI woes like acid reflux, bloating, and pain.
For one, slower eating often translates to more chewing. In addition to mechanically mashing food into a pulp, increased chewing also allows the mouth’s digestive enzymes to pre-digest food. As a result, the stomach and intestines have to work less hard.
Plus, eating in a relaxed setting often lowers stress hormones like norepinephrine and cortisol, making it less likely that they will intensify GI pain signals.
According to Maughan, this can be especially important for young parents, as it’s not always easy to eat undistracted and peacefully when tending to little ones.
(Sounds simple, but slow eating is more challenging than people think—and a lot more impactful. Learn more: Try the slow-eating 30-day challenge.)
IBS relief strategy #4: Troubleshoot sleep problems
According to research, people with IBS experience more shallow, less restorative, and more interrupted sleep.13
Because of poor sleep quality, many people with IBS sleep more hours overall than people without IBS—yet feel less rested.
Fatigue can then set off a vicious cycle. When people don’t sleep restfully, stress hormone levels tend to be higher, which can exacerbate gut pain.14
Unrested people also tend to feel hungrier during the day. Cravings for fats and sweets also intensify, driving people to reach for the very foods more likely to trigger IBS symptoms—and wolf them down too quickly.
Stopping this cycle can be challenging.
As with stress, you can’t simply will yourself to sleep more restfully.
However, the first three strategies—exercise, stress management, and slower eating—can all help.
Some PN clients have found that consuming a smaller dinner earlier in the evening gives their bodies more time to digest before bed. Other clients tell us that a relaxing pre-bedtime routine—a few minutes of foam rolling, a guided meditation, a bath, or some journalling—tends to help.
(Find out the best practices for getting better sleep by checking out our infographic: The power of sleep)
IBS relief strategy #5: Investigate your diet
While there’s no one-size-fits-all IBS diet, experts have identified several food categories that are more likely to be problematic for many people. These include:
Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAPs), which are a family of carbohydrate-rich foods that are poorly absorbed in the small intestine. Even in people without IBS, these foods tend to slow digestion and attract water. When gut bacteria ferment them, they produce gas, which can stretch the intestinal wall. For most, this slowed digestion and gas isn’t especially noticeable; In people with IBS, it can lead to intense pain. High-FODMAP foods include wheat, rye, barley, onions, garlic, beans, dairy, honey, cashews, some processed meats, and many fruits and vegetables. (More about FODMAPs in the next section.)
Caffeinated beverages and foods, especially coffee, which trigger the release of stress hormones, stimulate the production of stomach acid, increase muscle contractions in the colon, and irritate the lining of the intestine.15
Alcohol and spicy foods that irritate the gut.16 17
High fructose corn syrup and sugar alcohols such sorbitol and mannitol, which have been linked to gas, bloating, and diarrhea in susceptible people.18 19
Fatty, greasy foods, which can slow digestion and attract water, leading to loose stools, bloating, and gas.20 21
If the idea of giving up all the foods and beverages on the above list has you in a cold sweat, know this…
Not everyone with IBS is sensitive to the same foods and beverages.
“Everyone can have different triggers,” says Maughan. “That’s why it’s so important to figure out what makes your body feel good and what doesn’t.”
Some people struggle with apples but are okay with berries. Others can drink green tea but not black. One person might be able to consume five to eight ounces of beer but not 12. A gluten-free diet may work great for some but not others.
Similarly, many people find relief by avoiding certain high-FODMAP foods. However, you may only be sensitive to some FODMAPs and not others. If so, eliminating all FODMAPs would be unnecessarily restrictive and difficult to follow consistently.
For this reason, it can be helpful to try an elimination diet to see which foods and beverages are problematic—along with the quantities you can safely tolerate, says Maughan. You’ll learn more about elimination diets in the next section.
(Want someone to walk you through exactly how to do an elimination diet? Read: How and why to do an elimination diet.)
Scope of Practice: How to coach someone with IBS
In our online coaching communities, we often see people asking some version of the following question:
“My client just told me that she has IBS. Am I allowed to continue to coach this person?”
The answer: Yes, you certainly can.
As we mentioned, Maughan specializes in helping people with digestive problems. Coaching someone with IBS is no different than coaching a client with any other nutritional goal, she says.
“Because IBS is often largely associated with what someone eats, it’s within a coach’s wheelhouse—with some caveats,” says Maughan. “You can’t diagnose your client with the condition, and you should make it clear that you’re not prescribing a diet for them. In addition, you should encourage clients to seek care from a medical professional, especially if you suspect something other than IBS is going on.”
To stay within your scope of practice, follow these do’s and don’ts.
| DO | DON’T |
|---|---|
| Encourage clients with digestive issues to visit a healthcare professional so they can get a definitive diagnosis. | Tell clients, “It sounds like you might have IBS.” |
| Share information about potential lifestyle changes, including elimination diets. Help clients run experiments that allow them to gain insight about the connection between their lifestyle, diet, and their body. | Pitch a rigid and restrictive diet as a treatment that will cure all of the client’s digestive problems. |
| Offer to work with a client’s medical team. Help the client adopt and remain consistent with the lifestyle changes their team recommends. | Contradict medical professionals by telling clients that the medical establishment always gets IBS wrong. |
| Support clients with optional recipes and other tools that help them put what they learn about their body into practice. | Create a prescriptive anti-IBS meal plan for a client to follow. |
| Encourage clients to experiment with a multi-disciplinary approach to managing IBS so they can discover the right combination of approaches that works for them. | Tell clients that you have all the answers or that they don’t need to seek medical advice or therapies. |
| Ensure clients know they can choose to make any given lifestyle change—or not. | Use force or fear to manipulate clients into following your advice. |
Elimination diets for IBS: How and when to try them
Elimination diets do what the name suggests: They exclude certain foods for a short period—usually three weeks. Then, you slowly reintroduce specific foods and monitor your symptoms for possible reactions.
Elimination diets work a lot like a science experiment that helps you identify problematic foods.
The phrase “elimination diet” may sound scary and off-putting, as if you’ll be living for months on bland food you have to slurp through a straw.
However, there are many different types of elimination diets, with some much less restrictive than others.
Here are a few versions.
Elimination diet “lite” for IBS
This is an excellent option for people who suspect they already know which foods and beverages trigger symptoms.
It goes like this: You eliminate up to four foods for several weeks. Then, slowly reintroduce them one at a time to see if your symptoms return.
Let’s say, for example, from experience, you know you feel bad whenever you eat dairy. On the lite elimination diet, you’d eliminate just dairy for three weeks. Then you’d reintroduce it to see how you feel.
Elimination Diet “medium” for IBS
If you’re unsure of how food interacts with your GI tract—but aren’t ready for a super restrictive eating plan, our Precision Nutrition elimination diet is likely the way to go.
Created by PN and approved by several registered dietitians, the plan removes many of the foods most likely to cause problems, while still including a variety of vegetables, fruits, starches, legumes, nuts, seeds, and meats, so you can continue to eat a well-balanced diet.
To learn more, download our FREE Ultimate Guide to Elimination Diets. This ebook has everything you need to be successful, including an at-a-glance chart that helps you easily follow the diet, along with recipes, meal ideas, and tip sheets.
The FODMAP diet for IBS
Over several years, researchers at Monash University in Australia have developed and extensively studied a low-FODMAP elimination diet for people with IBS.22
Unlike other types of elimination diets, the FODMAP diet is a highly specialized form of medical nutrition therapy. The FODMAP diet’s list of problematic foods (shown below) is anything but intuitive, and the reintroduction phase is more complex than other elimination diets.
As a result, if you’ve been diagnosed with IBS and suspect you have a FODMAP issue, seek the expertise of a FODMAP-certified practitioner. You can also download Monash University’s FODMAP Diet app, which will help you navigate low-FODMAP eating.
| Food Group | Low FODMAP | High FODMAP |
|---|---|---|
| Vegetables | Green beans, bok choy, green bell peppers, carrots, cucumbers, lettuce, potatoes | Artichoke, asparagus, mushrooms, onions, garlic, snowpeas, cauliflower, leeks |
| Fruits | Cantaloupe, kiwi, mandarin, orange, pineapple, firm bananas, blueberries | Apples, cherries, mango, nectarines, peaches, pears, plums, watermelon, ripe bananas |
| Dairy and Dairy Alternatives | Almond milk, brie, feta, hard cheese, lactose-free milk & yogurt | Cow’s milk and foods made from cow’s milk, soy milk |
| Protein-Rich Foods | Eggs, tofu, tempeh, most minimally-processed meats, poultry, seafood | Most legumes, some marinated and processed meats |
| Starches | Foods made from oats, quinoa, rice, spelt, or corn | Foods made from wheat, rye, and barley |
| Sweeteners | Dark chocolate, maple syrup, rice malt, table sugar | High-fructose corn syrup, honey, sugar alcohols, agave |
| Nuts and Seeds | Peanuts, pumpkin seeds, almonds, macadamias, and walnuts | Cashews, pistachios |
The power of health coaching
In isolation, more knowledge doesn’t always lead to more power.
For example, there’s a difference between knowing that dairy messes with your gut and doing something with that knowledge.
Similarly, you might know that you feel better when you eat a small dinner earlier in the evening, but you may struggle to plan your life so an early dinner happens regularly.
This is where a certified health coach can help.
“Many of my clients already have an idea of the foods that tend to cause them problems,” says Maughan, “But they’re nervous to know for sure because they fear that the knowledge will make eating more challenging.”
That’s why Maughan assures clients…
Even if you do an elimination diet and you learn your favorite food is contributing to your IBS, you don’t have to do anything with that information.
You can choose to continue to eat your favourite foods if you want, AND you can choose to avoid them when it’s really important for you not to experience IBS symptoms, she says.
“With knowledge, you have choices,” says Maughan.
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
- Drossman, Douglas A., Carolyn Blank Morris, Susan Schneck, Yuming J. B. Hu, Nancy J. Norton, William F. Norton, Stephan R. Weinland, Christine Dalton, Jane Leserman, and Shrikant I. Bangdiwala. 2009. “International Survey of Patients with IBS: Symptom Features and Their Severity, Health Status, Treatments, and Risk Taking to Achieve Clinical Benefit‘.” Journal of Clinical Gastroenterology 43 (6): 541–50.
- Lacy, Brian E., Kelly K. Everhart, Kirsten T. Weiser, Ryan DeLee, Sebastian Strobel, Corey Siegel, and Michael D. Crowell. 2012. “IBS Patients’ Willingness to Take Risks with Medications.” The American Journal of Gastroenterology 107 (6): 804–9.
- Farndale R, Roberts L. Long-term impact of irritable bowel syndrome: a qualitative study. Prim Health Care Res Dev. 2011 Jan;12(1):52–67.
- Trindade IA, Melchior C, Törnblom H, Simrén M. Quality of life in irritable bowel syndrome: Exploring mediating factors through structural equation modelling. J Psychosom Res. 2022 Aug 1;159(110809):110809.
- Arif TB, Ali SH, Sadiq M, Bhojwani KD, Hasan F, Rahman AU, et al. S753 meta-analysis of global prevalence and gender distribution of irritable bowel syndrome (IBS) using Rome III and IV criteria. Am J Gastroenterol. 2024 Oct;119(10S):S517–S517.
- Riezzo G, Prospero L, D’Attoma B, Ignazzi A, Bianco A, Franco I, et al. The impact of a twelve-week moderate aerobic exercise program on gastrointestinal symptom profile and psychological well-being of irritable bowel syndrome patients: Preliminary data from a southern Italy cohort. J Clin Med. 2023 Aug 17;12(16):5359.
- Royes LFF. Cross-talk between gut and brain elicited by physical exercise. Biochim Biophys Acta Mol Basis Dis. 2020 Oct 1;1866(10):165877.
- Chiang H-L, Chuang Y-F, Chen Y-A, Hsu C-T, Ho C-C, Hsu H-T, et al. Physical fitness and risk of mental disorders in children and adolescents. JAMA Pediatr. 2024 Jun 1;178(6):595–607.
- Sohail MU, Yassine HM, Sohail A, Thani AAA. Impact of physical exercise on gut microbiome, inflammation, and the pathobiology of metabolic disorders. Rev Diabet Stud. 2019 Aug 4;15(1):35–48.
- Zhang L, Wang H-L, Zhang Y-F, Mao X-T, Wu T-T, Huang Z-H, et al. Stress triggers irritable bowel syndrome with diarrhea through a spermidine-mediated decline in type I interferon. Cell Metab. 2025 Jan 7;37(1):87-103.e10.
- Schaper SJ, Stengel A. Emotional stress responsivity of patients with IBS – a systematic review. J Psychosom Res. 2022 Feb 1;153(110694):110694.
- Staudacher HM, Black CJ, Teasdale SB, Mikocka-Walus A, Keefer L. Irritable bowel syndrome and mental health comorbidity – approach to multidisciplinary management. Nat Rev Gastroenterol Hepatol. 2023 Sep 2;20(9):582–96.
- Patel A, Hasak S, Cassell B, Ciorba MA, Vivio EE, Kumar M, et al. Effects of disturbed sleep on gastrointestinal and somatic pain symptoms in irritable bowel syndrome. Aliment Pharmacol Ther. 2016 Aug 30;44(3):246–58.
- Topan R, Vork L, Fitzke H, Pandya S, Keszthelyi D, Cornelis J, et al. Poor subjective sleep quality predicts symptoms in irritable bowel syndrome using the experience sampling method. Am J Gastroenterol. 2024 Jan 1;119(1):155–64.
- Koochakpoor G, Salari-Moghaddam A, Keshteli AH, Esmaillzadeh A, Adibi P. Association of coffee and caffeine intake with irritable bowel syndrome in adults. Front Nutr. 2021 Jun 15;8:632469.
- Reding KW, Cain KC, Jarrett ME, Eugenio MD, Heitkemper MM. Relationship between patterns of alcohol consumption and gastrointestinal symptoms among patients with irritable bowel syndrome. Am J Gastroenterol. 2013 Feb;108(2):270–6.
- Esmaillzadeh A, Keshteli AH, Hajishafiee M, Feizi A, Feinle-Bisset C, Adibi P. Consumption of spicy foods and the prevalence of irritable bowel syndrome. World J Gastroenterol. 2013 Oct 14;19(38):6465–71.
- Yao CK, Tan H-L, van Langenberg DR, Barrett JS, Rose R, Liels K, et al. Dietary sorbitol and mannitol: food content and distinct absorption patterns between healthy individuals and patients with irritable bowel syndrome. J Hum Nutr Diet. 2014 Apr;27 Suppl 2(s2):263–75.
- Suez J, Korem T, Zeevi D, Zilberman-Schapira G, Thaiss CA, Maza O, et al. Artificial sweeteners induce glucose intolerance by altering the gut microbiota. Nature. 2014 Oct 9;514(7521):181–6.
- Capili B, Anastasi JK, Chang M. Addressing the role of food in irritable bowel syndrome symptom management. J Nurse Pract. 2016 May;12(5):324–9.
- Simrén M, Agerforz P, Björnsson ES, Abrahamsson H. Nutrient-dependent enhancement of rectal sensitivity in irritable bowel syndrome (IBS). Neurogastroenterol Motil. 2007 Jan;19(1):20–9.
- De Giorgio R, Volta U, Gibson PR. Sensitivity to wheat, gluten and FODMAPs in IBS: facts or fiction? Gut. 2016 Jan 1;65(1):169–78.
If you’re a coach, or you want to be…
You can help people build sustainable nutrition and lifestyle habits that will significantly improve their physical and mental health—while you make a great living doing what you love. We’ll show you how.
If you’d like to learn more, consider the PN Level 1 Nutrition Coaching Certification. (You can enroll now at a big discount.)
The post Over a Tenth of Your Clients Are Dealing With IBS—And Here’s How to Help appeared first on Precision Nutrition.
Source: Health1
Reviewed by Brian St. Pierre, MS, RD and Helen Kollias, PhD
It’s like my thoughts were under a pile of garbage.
On a Friday night, as my husband and I tried to figure out where to eat, a typical conversation would go like this:
Me: Do you want to go to that restaurant?
Him: What restaurant?
Me: I can’t think of the name. We’ve eaten there before. It’s that place with the peanut shells on the floor? It’s next to… You know… It’s on that road where we used to take the dog to the vet. Do you know the one I’m talking about??
It was as if certain details got lost in a pile of sludge in the deep recesses of my brain. Then, hours later, the details would escape, and I’d shout into an empty room…
“Texas Roadhouse!”
Sludginess with proper nouns is typical for people who are middle-aged and beyond.
However, what seemed to be happening to me, increasingly in my late 40s and early 50s, felt far from typical.
Not only could I never seem to spit out the names of various restaurants or people or books or movies or so many other things, but my brain was also pooping out during the workday.
I’d sit in front of my computer screen, stare at a document, and will myself to do something constructive with my fingertips. Everything seemed hazy, like those first few moments in the morning when you’re awake enough to turn off the alarm but too sleepy to do basic math.
I had my good moments, usually in the morning, when I attempted to pack eight hours of writing into the two or three hours I possessed mental clarity.
On my worst days, however, I awoke with a haze I never managed to shake. Work was a non-starter. Nor did I have enough bandwidth to read, or do much of anything, really.
I sought medical advice.
Three healthcare professionals recommended antidepressants. I tried one, and felt even worse. I tried another. I tried yet another at a higher dose. Still, I felt like a zombie. Another professional gave me a sleeping pill. It left me feeling even more drugged.
Someone tested my thyroid. There was nothing wrong with it. Nor was I anemic. I tried supplements, mushroom coffee, and just about any product with the word “think” somewhere on its label.
Finally, after nearly two years of seeing a revolving door of doctors, I made an appointment with a gynecologist for my yearly exam. I mentioned vaginal dryness. That information triggered her to ask a string of questions that had nothing to do with my undercarriage. How was my sleep? Mood? Energy levels? Was I experiencing hot flashes? How about brain fog?
“Funny you should mention brain fog,” I said in my usual hazy monotone. “I feel like I’m barely alive.”
By the end of the visit, I understood that I’d likely never had depression.
What I “had” was menopause.
My gynecologist sent me home with prescriptions for estradiol and progesterone.
Within days, it was as if someone had flipped a switch.
I could think again. I could type words again. I could follow conversations. I could work past noon.
And, for the first time in years, I could sleep more than two hours without waking.
Now, menopause isn’t a medical condition.
Nor is it a disease.
Instead, like puberty, it’s a life stage—a transitional moment to be precise.
Once you’ve gone 12 consecutive months without a period, you’ve reached menopause. And from that moment onwards, you’re officially “postmenopausal.”
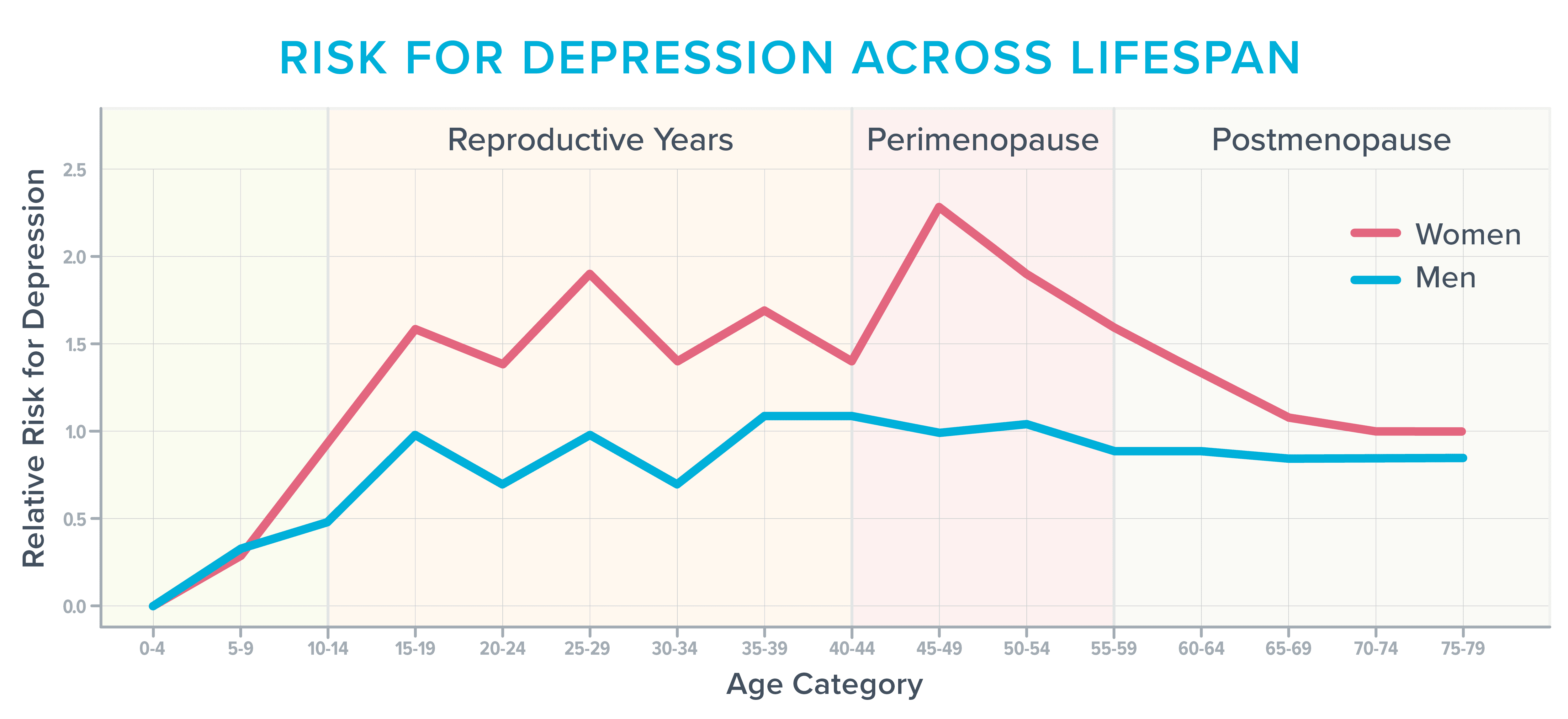
As women approach this transitional moment, hormone levels fluctuate and fall, triggering dozens of symptoms. Weight gain and reduced sex drive get a lot of attention.
However, during and after menopause, roughly 40 percent of women report increased irritability, mood swings, anxiety, fatigue, and trouble concentrating, according to the American College of Obstetricians and Gynecologists.1 2 As the following image shows, it’s also one of the most vulnerable times in a woman’s life to develop depression,3 particularly if they’ve struggled in the past with it before.
Before starting hormones, I often found myself sobbing for no reason. Other times, the world’s stimuli felt too… stimulating.
Normal everyday sounds—like the buzz of traffic or people at the mall—literally hurt. I was jumpy and irritable and felt anxious about situations that had never bothered me in the past, such as driving over bridges or through construction.
It’s not completely clear what drives these cognitive and emotional symptoms.
Fluctuating hormone levels likely play a role, as do typical age-related changes in the brain.
In addition, during this stage of life, women often deal with several issues that siphon cognitive capacity faster than a thirsty vampire drains a carotid.
During their 40s and 50s, for example, many women have reached the peak of their careers, with responsibilities that follow them home and keep them up at night. They may also be parenting angst-filled teens, caring for aging parents, adjusting to an empty nest, questioning their marriage, or trying to wrap their bank account around the latest statement from the college bursar or hospital billing department.
However, one of the lesser-known and talked about triggers for cognitive discontent has nothing to do with aging or life stress and everything to do with that hallmark menopausal symptom: the hot flash.
Anatomy of a hot flash
Hot flashes, which happen during the day, and night sweats, which occur at night, fall under the category of vasomotor symptoms. (The word “vasomotor” refers to the constriction or dilation of blood vessels which, in turn, can influence everything from blood pressure to sweating.)
During a hot flash or night sweat, norepinephrine and cortisol levels rise. Blood vessels dilate in an attempt to shed heat. Blood pressure and heart rate increase.
Depending on the severity of the hot flash, your skin might redden as sensations of warmth spread through your face, neck, and chest.
You might sweat, experience heart palpitations, or feel anxious, tired, or faint.4
It’s not entirely clear why hot flashes crop up around menopause.
According to one theory, falling estrogen levels affect the hypothalamus, the area of the brain involved in temperature regulation. The brain’s internal thermostat gets wonky and occasionally thinks your body is too hot or cold (when it’s not).
How vasomotor symptoms change the brain
For many years, experts thought of vasomotor symptoms as mere inconveniences or sources of embarrassment.
(To be honest, so did I. During all of those fruitless visits to various healthcare professionals, it never occurred to me to mention them.)
However, an increasing body of research has revealed that hot flashes may do more than make us uncomfortable or force us to change our sheets in the middle of the night.
They may also affect our blood vessels and brains—and not for the better.5 For this reason, an increasing number of experts now consider vasomotor symptoms to be a treatable medical condition.6 7 8
Hot flashes and brain lesions
In one study, researchers asked 226 women to wear monitors that tracked when they were experiencing a hot flash. The women also underwent magnetic resonance imaging (MRI), filled out sleep diaries, and wore smartwatches that recorded how often they woke at night.9
As researchers looked at the brain images obtained from women who experienced the most hot flashes, they noticed an abundance of patchy areas called whole-brain white matter intensities.
These lesions were once thought of as a typical consequence of aging. However, neuroscientists now believe that the presence of whole-brain white matter intensities is predictive of future cognitive decline.
People with an abundance of these brain lesions are twice as likely to get diagnosed with dementia and three times as likely to have a future stroke.10
The blood vessel connection
It’s thought that the increased presence of whole-brain white matter intensities may stem, in part, from changes taking place in the blood vessels that feed the brain.
A three-year study of 492 women supports that theory. It determined that women who experienced frequent hot flashes also tended to experience unhealthy changes in their blood vessels, such as an inability to dilate to accommodate increased blood flow.11
Other research has linked frequent hot flashes with increases in the following:
- Thickening in the carotid arteries that supply blood to the brain, face, and neck12
- Body fat
- Total and LDL cholesterol
- Insulin resistance13 14 15 16
The sleep connection
In addition to directly affecting the blood vessels, frequent hot flashes may also affect the brain by disturbing sleep.17
Interestingly, many women don’t necessarily know that hot flashes are disturbing their sleep.
They may instead—as I did—assume they have insomnia or sleep apnea.
That’s because night sweats aren’t always sweaty.
By the time a surge in cortisol and norepinephrine jolts a woman awake, the hotness of the flash may have dissipated. So, it can feel as if she’s repeatedly waking, over and over and over again, for no discernable reason.
These frequent awakenings may interfere with the brain’s ability to consolidate memories, metabolize toxins, and store all the names, dates, and facts one encounters daily.
It can also lead to lost connectivity in the hippocampus, a part of the brain that’s important for learning and memory.
Sleep loss also means the amygdala, a part of the brain involved in emotion, becomes more reactive, causing people to feel more easily stressed, anxious, irritable, frustrated, or enraged.18 19
All of these brain changes can set in after just days to a week of lost sleep. So, imagine what happens when you’ve been waking over and over again—for years.
Why it can be hard to get help
To diagnose depression, healthcare professionals use a tool called the Patient Health Questionnaire (PHQ-9) depression scale. If you check off four of the nine symptoms on the scale, you’re considered depressed.
However, four of the symptoms on the checklist also overlap with the symptoms of menopause-related sleep deprivation:
- Little interest or pleasure in doing things
- Trouble falling or staying asleep
- Feeling tired or having little energy
- Trouble concentrating on things, such as reading the newspaper or watching television
Check off those four items, and you might be diagnosed with depression, even if what’s really ailing you is the battle with sleep you’ve been waging since you turned 47.
A lack of menopause-specific training
Another problem: On surveys, 80 percent of medical residents admit they feel “barely comfortable” talking about menopause.20 In addition, few residency programs—including ob-gyn residency programs—offer training in it.21
Given the above, it’s no wonder so many healthcare professionals never think to ask about hot flashes or sleep disturbances when people like me show up complaining of fatigue, lack of gumption, and an inability to focus.
In addition, even when it’s clear that vasomotor symptoms are leading to cognitive and emotional symptoms, many healthcare professionals still shy away from prescribing menopausal hormone therapy (also called hormone replacement therapy, or HRT), often telling women that supplemental hormones are “not safe” or “too risky.”
These professionals are practicing what Michigan-based menopause-trained gynecologist Jerrold H. Weinberg, MD, calls “defensive medicine.”
“It’s one of the first reflexes doctors have when they recommend a treatment,” says Dr. Weinberg. “They worry they’re going to get sued.”
What the research actually says about hormone therapy
These worries are based on research done several decades ago that linked the use of certain types of hormones with a slightly increased risk of developing breast cancer or stroke.22
However, according to more recent research, that small increased risk seems to depend on several other factors, such as age, dose, the type of hormonal preparation, and the duration of hormone use.23 24
As long as you’re younger than 60 and have been postmenopausal for fewer than 10 years, many experts now say the benefits outweigh the risks for women with moderate to severe menopausal symptoms.25
It’s also counterbalanced by health benefits such as reduced risk of developing Alzheimer’s disease or osteoporosis, says Dr. Weinberg, who confirms the health benefits of menopause hormone therapy far outweigh the risks for most women.
Because some antidepressants can lift mood, improve sleep, and reduce hot flashes, some healthcare professionals turn to them instead of menopause hormone therapy. As with any medicine, antidepressants have their own list of side effects. However, for someone practicing defensive medicine, they often seem like a safer bet, says Dr. Weinberg.26 27 28
How to advocate for your health
If you or your client are on what seems like a never-ending quest to find a healthcare professional who understands menopause, use the following advice from Dr. Weinberg and Helen Kollias, PhD, an expert on physiology and molecular biology and science advisor at Precision Nutrition and Girls Gone Strong.
Seek care from a menopause-trained health professional.
Usually, these professionals list this training and interest in their bio. For example, they might list “menopause” as an area of focus.
You can also search this database for practitioners who have earned a certification from the Menopause Society.
Document your symptoms.
Write them down. That way, if you feel foggy or nervous during your appointment, you can lean on your notes.
This information can also help you judge whether MHT or another medicine is working. Based on your symptom data, you and your healthcare professional may decide to switch to a different medicine or change your dose.
Consider tracking:
- How often you get hot flashes
- The number of hours in a typical day you find yourself battling brain fog
- How often you experience fatigue, anxiety, rage, or some other symptom
- How often you wake up at night
Be as specific as you can during your appointment.
Saying something like “I don’t sleep well,” is less likely to get you the right kind of help than saying, “During the past seven days, I’ve only gotten four uninterrupted hours once. I wake, on average, five times a night. On a typical night, my longest stretch of sleep is three hours.”
If you use a smartwatch, come ready to fire up your health app, so your healthcare professional can see the data.
Talk about the pros and cons of treatment.
There’s a concept in medicine known as “shared decision-making.” Part of that process involves frank discussions about the benefits and risks of a given treatment. Then, patients and clinicians work together to make decisions based on those benefits and risks.
Many healthcare networks encourage clinicians to use shared decision-making, as it seems to reduce patient complaints as well as malpractice lawsuits.29 30
For this reason, shared decision-making can help shift a healthcare professional out of the “defensive medicine” mindset.
You might ask questions like:
- “I’m interested in seeing if menopausal hormone therapy might be helpful. Could we discuss if I’m a good candidate?”
- “I’ve read that menopausal hormone therapy could slightly increase my risk of breast cancer. Could you help me understand my personal breast cancer risk based on my family history, age, body weight, and lifestyle?”
- “Osteoporosis runs in my family, as does dementia. I’ve heard that menopausal hormone therapy might help to reduce the risk for both, in addition to helping me sleep. Could you help me weigh the pros and cons?”
How to improve mental and emotional health during menopause: 9 lifestyle strategies
The lifestyle habits that improve mental and emotional health during menopause aren’t terribly different from the lifestyle habits that improve overall health—for any person, at any stage of life.
Other than avoiding caffeine, alcohol, and spicy or hot foods, there’s no special diet for people with vasomotor symptoms. (And by the way, tofu and other soy products don’t seem to help with vasomotor symptoms as much as once thought30—though they’re still nutritious.)
Strategy #1: Lean into fundamental health strategies.
Healthy behaviors don’t necessarily change during middle age.
Nutrition, physical activity, stress management, sleep, social connectedness, and a sense of purpose matter just as much during the menopausal transition as they do when we’re younger. However, these fundamentals are even more important to dial in as life progresses.
So consider:
- Are you setting aside enough time for sleep and rest?
- Are you physically active?
- Are you eating a diet that’s mostly minimally processed and full of brightly colored produce, healthy fats, lean protein, fibrous vegetables, and legumes?
- Do you regularly connect with other humans in ways that help you buffer stress and feel supported?
- Do you find ways to experience awe, joy, curiosity, peace, and purpose?
If you answered “no” to some or all of those questions, consider why that is. What’s stopping you? How might you remove barriers or shore up support to make those fundamentals easier?
Strategy #2: Experiment with creatine.
In addition to helping to blunt age- and hormone-related losses in muscle and bone mass, creatine may also help bolster mood and brain function while reducing mental fatigue.
It also seems to counter some of the negative effects of sleep deprivation. 32 33 Research shows a daily dose of 5 to 7 grams of creatine monohydrate is effective.
Strategy #3: Get regular about light exposure.
In addition to helping you feel alert, sunlight helps to set the internal clock in your brain that makes you sleepy at night and spunky in the morning. Morning and late afternoon light exposure seem particularly potent.
In a study of 103 people, exposure to morning sunlight predicted better sleep quality the following night. When people spent time outdoors in the mornings, they fell asleep more quickly, slept longer, and experienced fewer awakenings the following evening.34
Sunlight may also improve mood and concentration.35
Strategy #4: Go easier at the gym.
If you’re already worn out, long, intense exercise sessions will likely make you feel worse.
For one, injuries crop up much more easily at middle age than during our 20s and 30s. In addition, it takes longer to recover between sessions.36
String too many overly zealous workouts too close together, and you’ll not only likely start to feel achy but also more irritable, tense, and tired.
However, much like a cold shower, short bursts of exercise may help you to feel alert during the day.
If you’re falling asleep at your desk, encourage yourself to take short movement breaks such as a 5- or 10-minute walk outdoors or a quick set of pushups or squats.
In addition, you may find gentle exercise—such as yoga or stretching—helps you relax before bed. Just don’t make it too intense, or you’ll trigger a release of adrenaline.
Whenever you exercise, tune into how your body feels, especially after a particularly bad night of sleep.
We’re not saying you should never exercise vigorously or try to beat your lifting PRs. However, depending on your sleep and recovery, you might want to pare things back, especially if you’ve traditionally hit the gym hard.
You can still do intense sessions—just balance them out with more moderate sessions, as well as proportionate recovery.
Depending on how you feel, you might decide to go all out, as usual.
However, you might also decide to do a zone 2 training session instead of an intense run. Or, if you’re resistance training, you might still do your planned session, but reduce the number of sets, reps, or volume lifted.
Strategy #5: Investigate Cognitive Behavior Therapy for Insomnia (CBT-I).
This research-based therapy for insomnia can help you develop skills and mental reframes that encourage sound sleep.
For example, a CBT-I therapist will help you develop the skill of getting up at the same time every day, regardless of how badly you slept (or didn’t sleep) the night before.
(Read more: Three CBT-I skills that can transform how you sleep.)
Strategy #6: Get real about stress.
You may not have the energy (or desire) to do everything you did when you were younger. (When you were 36, your daily checklist defied time and space.)
As a result, you might benefit from looking critically at your current responsibilities to see which ones you can shrink or downsize. For several days, track how you spend your time and bandwidth. Then, analyze your data.
Ask yourself:
- Is this how you truly want to spend your time and energy?
- Does your current schedule allow you to rest, recover, and tend to your own needs? Or, do you spend nearly all of your time and energy caring for and providing for others?
- What changes could you make to prioritize rest and recovery?
If you’re a coach, use the Wheel of Stress Assessment to help clients identify different dimensions of their life that might be draining their mental and emotional capacity. (When you know specifically where your stress is coming from, you have a better chance of resolving it.)
If it’s demands from other people that prevent you from prioritizing self-care and recovery, you might like to read: How saying “no” can seriously change your life.
Strategy #7: Experiment with cooling technology.
You might find you sleep better and experience fewer night sweats if you sleep in a cooler environment.
Try turning down the thermostat a couple of degrees, using a fan, or investing in an electric cooling mattress pad.
Strategy #8: Take frequent breaks.
When you feel the fog take over your brain, it’s not likely you’ll be doing “your best work” anyway.
So, for a block of time—say, 20 minutes—permit yourself to do nothing. You might:
- Relax with a cold beverage
- Cuddle with a pet
- Gaze out a window
- Sit outdoors while listening to the birds
- Call a friend
If you need a quick “refresh,” you can also try a 5-minute mind-body scan.
Get your body into a comfortable position. For example, you might use the yoga “legs up the wall” pose or lie down and place a pillow under your knees.
Then, close your eyes and bring your attention to physical sensations in your body. Start at your head, and work your way down to your toes.
Don’t judge or rush to change anything. Just observe, like a scientist. You can also scan your mind, for example, by noticing thoughts.
When you’ve completed the scan, consider:
- What are you feeling physically?
- What are you feeling emotionally?
- What are you thinking?
You don’t have to “do” anything with the information you uncover, just notice.
Strategy #9: Follow a diet that promotes healthy circulation.
The foods that protect the blood vessels around your heart can also protect the blood vessels in your brain.
For example, both the MIND and Mediterranean diets are associated with a reduced risk of Alzheimer’s disease and depression.37 38 These eating patterns are rich in vegetables, fruit, whole grains, olives, beans, fish, and other minimally-processed whole foods.
In addition, nitrate-rich foods like beets and dark, leafy greens may help to dilate blood vessels, temporarily improving memory by helping more blood to reach the brain.39 40
(For more on how our diet can support brain function and emotional regulation, read: Nutrition and mental health: What (and how) to eat)
The upside of menopause
It’s frustrating when you feel like you can’t do it all.
Believe me. I know.
However, this stage of life presents a hidden opportunity, forcing you to re-evaluate what’s most important.
Before going on hormones, as my ability to type coherent words and phrases diminished, I was forced to ask an important question:
Do I really need to be doing this?
It was more of an existential question than a career-related one, and it allowed me to reassess how I wanted to spend my limited mental resources.
Given that I was self-employed, I didn’t actually need to be working eight hours a day. That was a gift, wasn’t it?
Maybe I also didn’t need to cook dinner six nights out of seven. Maybe the recipes I chose could be simplified, too.
Finally, maybe saying “no” a lot more often and without regret would allow me to continue to say yes to the things that mattered most.
Things like visiting my aging parents.
And picking up the phone whenever my kid called from college.
Or meeting a friend for a meandering walk around town.
Thanks to the hormones and life tweaks, I now have energy again. I’m also clear-headed most of the time. However, I still tend to end my work day around 3 p.m.
Why?
Because I can, and I want to.
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
- Mood Changes During Perimenopause Are Real. Here’s What to Know [Internet]. [cited 2024 Nov 1]. Available from: https://www.acog.org/womens-health/experts-and-stories/the-latest/mood-changes-during-perimenopause-are-real-heres-what-to-know
- Gordon JL, Eisenlohr-Moul TA, Rubinow DR, Schrubbe L, Girdler SS. Naturally occurring changes in estradiol concentrations in the menopause transition predict morning cortisol and negative mood in perimenopausal depression. Clin Psychol Sci. 2016 Sep;4(5):919–35.
- N.d. Accessed November 20, 2024. https://nap.nationalacademies.org/read/27757/chapter/8.
- Lugo T, Tetrokalashvili M. Hot flashes. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
- Andrews R, Lacey A, Bache K, Kidd EJ. The role of menopausal symptoms on future health and longevity: A systematic scoping review of longitudinal evidence. Maturitas. 2024 Sep 30;190(108130):108130.
- Thurston RC, Chang Y, Wu M, Harrison EM, Aizenstein HJ, Derby CA, et al. Reproductive hormones in relation to white matter hyperintensity volumes among midlife women. Alzheimers Dement. 2024 Sep;20(9):6161–9.
- Thurston RC, Maki P, Chang Y, Wu M, Aizenstein HJ, Derby CA, et al. Menopausal vasomotor symptoms and plasma Alzheimer disease biomarkers. Am J Obstet Gynecol. 2024 Mar 1;230(3):342.e1-342.e8.
- Thurston RC, Wu M, Barinas-Mitchell E, Chang Y, Aizenstein H, Derby CA, et al. Carotid intima media thickness and white matter hyperintensity volume among midlife women. Alzheimers Dement. 2023 Jul;19(7):3129–37.
- Thurston RC, Wu M, Chang Y-F, Aizenstein HJ, Derby CA, Barinas-Mitchell EA, et al. Menopausal vasomotor symptoms and white matter hyperintensities in midlife women. Neurology. 2023 Jan 10;100(2):e133–41.
- Wardlaw JM, Valdés Hernández MC, Muñoz-Maniega S. What are white matter hyperintensities made of? Relevance to vascular cognitive impairment: Relevance to vascular cognitive impairment. J Am Heart Assoc. 2015 Jun 23;4(6):001140.
- Thurston RC, Sutton-Tyrrell K, Everson-Rose SA, Hess R, Matthews KA. Hot flashes and subclinical cardiovascular disease: findings from the Study of Women’s Health Across the Nation Heart Study: Findings from the Study of women’s Health Across the Nation Heart Study. Circulation. 2008 Sep 16;118(12):1234–40.
- Thurston RC, Chang Y, Barinas-Mitchell E, Jennings JR, Landsittel DP, Santoro N, et al. Menopausal Hot Flashes and Carotid Intima Media Thickness Among Midlife Women. Stroke. 2016 Dec;47(12):2910–5.
- Thurston RC, Sowers MR, Sternfeld B, Gold EB, Bromberger J, Chang Y, et al. Gains in body fat and vasomotor symptom reporting over the menopausal transition: the study of women’s health across the nation. Am J Epidemiol. 2009 Sep 15;170(6):766–74.
- Thurston RC, El Khoudary SR, Sutton-Tyrrell K, Crandall CJ, Gold EB, Sternfeld B, et al. Vasomotor Symptoms and Lipid Profiles in Women Transitioning Through Menopause. Obstetrics & Gynecology. 2012 Apr;119(4):753–61.
- Thurston RC, El Khoudary SR, Sutton-Tyrrell K, Crandall CJ, Sternfeld B, Joffe H, et al. Vasomotor Symptoms and Insulin Resistance in the Study of Women’s Health Across the Nation. The Journal of Clinical Endocrinology & Metabolism. 2012 Oct;97(10):3487–94.
- Thurston RC, Chang Y, Barinas-Mitchell E, Jennings JR, von Känel R, Landsittel DP, et al. Physiologically assessed hot flashes and endothelial function among midlife women. Menopause. 2017 Aug;24(8):886–93.
- Thurston RC, Chang Y, Buysse DJ, Hall MH, Matthews KA. Hot flashes and awakenings among midlife women. Sleep [Internet]. 2019 Sep 6 [cited 2024 Oct 31];42(9). Available from: https://pubmed.ncbi.nlm.nih.gov/31152182/
- Roy S. Sleep Deprivation Harms Memory Via Loss of Connectivity Between Hippocampus Neurons [Internet]. Sleep Review. 2016 [cited 2024 Oct 31]. Available from: https://sleepreviewmag.com/sleep-health/demographics/age/sleep-deprivation-harms-memory-via-loss-connectivity-hippocampus-neurons/
- Minkel JD, Banks S, Htaik O, Moreta MC, Jones CW, McGlinchey EL, et al. Sleep deprivation and stressors: evidence for elevated negative affect in response to mild stressors when sleep deprived. Emotion. 2012 Oct;12(5):1015–20.
- Dorr B. Contributor: In the Misdiagnosis of Menopause, What Needs to Change? [Internet]. AJMC. 2022 [cited 2024 Oct 31]. Available from: https://www.ajmc.com/view/contributor-in-the-misdiagnosis-of-menopause-what-needs-to-change-
- Allen JT, Laks S, Zahler-Miller C, Rungruang BJ, Braun K, Goldstein SR, et al. Needs assessment of menopause education in United States obstetrics and gynecology residency training programs. Menopause. 2023 Oct 1;30(10):1002–5.
- Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA. 2002 Jul 17;288(3):321–33.
- Nerattini M, Jett S, Andy C, Carlton C, Zarate C, Boneu C, et al. Systematic review and meta-analysis of the effects of menopause hormone therapy on risk of Alzheimer’s disease and dementia. Front Aging Neurosci. 2023 Oct 23;15:1260427.
- Gosset A, Pouillès J-M, Trémollieres F. Menopausal hormone therapy for the management of osteoporosis. Best Pract Res Clin Endocrinol Metab. 2021 Dec;35(6):101551.
- Garrison JA. UpToDate. J Med Libr Assoc. 2003;91(1):97.
- Newhouser LM, Maneval M, Rayalam K, Sabeeh G, Varela L. SSRIs vs. SNRIs for vasomotor symptoms of menopause. Am Fam Physician. 2022 Apr;105(4):430–1.
- Wu C-K, Tseng P-T, Wu M-K, Li D-J, Chen T-Y, Kuo F-C, et al. Antidepressants during and after menopausal transition: A systematic review and meta-analysis. Sci Rep. 2020 May 15;10(1):8026.
- Schoenfeld EM, Mader S, Houghton C, Wenger R, Probst MA, Schoenfeld DA, et al. The effect of shared decisionmaking on patients’ likelihood of filing a complaint or lawsuit: A simulation study. Ann Emerg Med. 2019 Jul 3;74(1):126–36.
- US Preventive Services Task Force, Davidson KW, Mangione CM, Barry MJ, Nicholson WK, Cabana MD, et al. Collaboration and shared decision-making between patients and clinicians in preventive health care decisions and US Preventive Services Task Force recommendations. JAMA. 2022 Mar 22;327(12):1171–6.
- Gençtürk N, Bilgiç FŞ, Kaban HU. The effect of soy isoflavones given to women in the climacteric period on menopausal symptoms and quality of life: Systematic review and meta-analysis of randomized controlled trials. Explore (NY). 2024 May 22;20(6):103012.
- Smith-Ryan AE, Cabre HE, Eckerson JM, Candow DG. Creatine Supplementation in Women’s Health: A Lifespan Perspective. Nutrients [Internet]. 2021 Mar 8;13(3).
- Gordji-Nejad A, Matusch A, Kleedörfer S, Jayeshkumar Patel H, Drzezga A, Elmenhorst D, et al. Single dose creatine improves cognitive performance and induces changes in cerebral high energy phosphates during sleep deprivation. Sci Rep. 2024 Feb 28;14(1):4937.
- Anderson AR, Ostermiller L, Lastrapes M, Hales L. Does sunlight exposure predict next-night sleep? A daily diary study among U.S. adults. J Health Psychol. 2024 Jul 30;13591053241262643.
- Burns AC, Windred DP, Rutter MK, Olivier P, Vetter C, Saxena R, et al. Day and night light exposure are associated with psychiatric disorders: an objective light study in >85,000 people. Nat Ment Health. 2023 Oct 9;1(11):853–62.
- Li DCW, Rudloff S, Langer HT, Norman K, Herpich C. Age-Associated Differences in Recovery from Exercise-Induced Muscle Damage. Cells [Internet]. 2024 Jan 30;13(3).
- Agarwal P, Leurgans SE, Agrawal S, Aggarwal NT, Cherian LJ, James BD, et al. Association of Mediterranean-DASH Intervention for Neurodegenerative Delay and Mediterranean diets with Alzheimer disease pathology. Neurology. 2023 May 30;100(22):e2259–68.
- Wightman EL, Haskell-Ramsay CF, Thompson KG, Blackwell JR, Winyard PG, Forster J, et al. Dietary nitrate modulates cerebral blood flow parameters and cognitive performance in humans: A double-blind, placebo-controlled, crossover investigation. Physiol Behav. 2015 Oct 1;149:149–58.
- Ventriglio A, Sancassiani F, Contu MP, Latorre M, Di Salvatore M, Fornaro M, Bhugra D. Mediterranean Diet and its Benefits on Health and Mental Health: A Literature Review. Clin Pract Epidemiol Ment Health. 2020 Jul 30;16(Suppl-1):156–164
- Heiland EG, Lindh F, Regan C, Ekblom Ö, Kjellenberg K, Larsen FJ, et al. A randomised crossover trial of nitrate and breakfast on prefrontal cognitive and haemodynamic response functions. Npj Sci Food. 2024 Sep 13;8(1):64.
The post Menopause and mental health: The science of the menopausal brain appeared first on Precision Nutrition.
Source: Health1
“I work with coaches and other people who know too much.”
Kate Solovieva is a former professor of psychology, a PN master coach, and PN’s director of community engagement.
And the above quote has become one of her taglines.
Though Coach Kate has coached thousands of “regular” clients, her specialty is coaching other coaches.
Through her work as an instructor with PN’s Level 2 Master Health Coaching Certification, a facilitator for PN’s private online coaching communities, and a coach in her own private practice, she gets a front-row view of all the questions and challenges both new and seasoned coaches have.
Coach Kate knows what other coaches are up to.
She’s seen the victories and the blunders of thousands of coaches, and today, she’ll share three common mistakes she sees them making.
If there’s anything Coach Kate wants, it’s to see her peers achieve wild success, so her hope with this article is to help coaches:
- Stop feeling paralyzed by insecurity and doubt—and start growing their business
- Learn to see their clients more objectively, so they can best serve their needs and goals
- Clearly identify their responsibilities as a coach (hint: they’re’ not what many coaches think they are)
- Harness their natural passion and investment in a client’s success—without burning themselves out
We’ll cover three common coaching mistakes, plus the solutions to overcome them. Let’s get into it.
Coaching mistake #1: Focusing on coaching instead of selling
Coach Kate describes a coaching business as a three-legged stool.
- There’s the coaching leg (which is your skills and knowledge as a coach),
- A selling leg (which is your ability to market and attract a flow of clients), and
- An administrative leg (which includes how clients book appointments, make payments, and other organizing tools and systems).
“The vast majority of folks who get into coaching start with the coaching leg,” says Kate.
“They want to become the best coach they can be, which is amazing. However, to become the best coach you can be, information and theory only get you so far.”
As Kate says, “You cannot become the best coach you can be in a vacuum, talking to yourself in your office.”
Which is why she suggests challenging the desire many coaches have to wait until their knowledge is “complete.”
Instead, she suggests, just start selling.
Why?
Coaches who start selling sooner also get to start coaching sooner.
Over time, they’ll have an advantage over the coaches who want to be “the BEST coach they can be” by getting 12 certifications before selling their services.
Meanwhile, the coach who “doesn’t really know what they’re doing” but has started practicing anyway will begin building their business and their coaching experience—and likely improve their odds of overall success.
Solution: Remember to show up as a COACH, not an EXPERT
There’s a natural inclination among aspiring coaches who want to do a good job to get those 12 certifications before they start coaching.
“Sometimes we hold on to this hope that we’ll get to a point where we feel confident enough at fielding any question that ever comes our way,” Kate says.
Because as every coach knows, when you start telling people what you do, they’ll have questions. And often, they’ll have questions you can’t answer, and that can feel uncomfortable… mortifying even.
(You’re supposed to be the expert, right??)
According to Coach Kate, the above belief—that you’re supposed to be an authority with all the answers—is based on an erroneous assumption.
“When I show up to a coaching conversation, my role is not ‘the expert,’” she says.
Yes, coaches have to show up to client interactions with a baseline of nutrition knowledge. (For example, if a client asks you about good sources of protein, you should be able to list some.)
But coaches don’t have to show up with a prepared lecture, or encyclopedic knowledge of nutrition minutia or biochemistry. (You don’t have to feel bad if you can’t recall the ratio of omega 3 to omega 6 in flax oil, or all the steps in the Krebs cycle that produces ATP.)
Even when you know the answer, Kate suggests that not answering right away can actually be more productive.
“If a client asks you about seed oils, you can simply say, ‘That’s a great question. I can get you some information on that if you’d like, but I’m curious, why do you ask?’”
While the expert might respond with a summary of the latest research on seed oil processing and its health effects, the coach will strive to learn more about why the question is meaningful to the client.
For example, after inquiring further, you may learn that your client heard about seed oils from their friend Susan, who changed the fat sources in her diet and lost ten pounds. And the client is curious to see if they might also lose ten pounds if they eliminate seed oils.
With this kind of response, you learn more about what the client is really after (a weight loss solution), which ultimately helps direct you to more effective strategies (which probably have nothing to do with seed oils).
Takeaway nugget:
Coaches should have a firm understanding of fitness and nutrition principles.
However, clients often don’t need more information; they need coaching.
When a client asks you a question, consider whether the answer will help them take action.
If it will, offer them what you know. (If you don’t know the answer, you can simply say, “I’m happy to find more information about that for you.”)
If it won’t, consider turning their question into a coaching opportunity. Ask, “Can you tell me why you’re curious about that?” Their answers will likely lead you to a more productive conversation.
Coaching mistake #2: Assuming your clients are exactly like you
Now, maybe it sounds obvious that clients aren’t just clones of us.
That said, especially when we feel all warm and vibe-y with our clients, it can be easy to forget in the moment.
For example, maybe you’re someone who…
- Tracks macros, and feels it’s relatively simple and effective. So you assume this approach will work on most clients (even though many will find it triggering and overwhelmingly complicated).
- Coaches virtually, so your clients are all over the world. You might recommend meeting certain protein targets, without considering that in some communities, protein dense foods might either be hard to access, prohibitively expensive, or both.
- Prioritizes fitness. And for the life of you, you can’t understand why your client would skip a lunch workout because she doesn’t want to mess up her hair and makeup in the middle of a work day.
If you’re a coach, you probably went into this line of work because you value nutrition, exercise, and overall health. And often, we assume our clients hold these same values. But the truth is, that’s not always the case.
Says Kate:
“There’s nothing inherently superior about valuing your health. If you do, yes, you’ll probably experience better health and live longer. But not everyone shares those values. That’s a tough one to swallow.”
Of course, without seeing your clients for the unique people they are—with their own individual preferences, values, and goals—you may find yourself suggesting behaviors that aren’t possible for them, or striving for goals that aren’t meaningful to them.
Over time, this becomes frustrating for your clients and you: They feel like you don’t “get” them, and you feel like a “bad” coach.
Solution: Get a clear picture of the client’s baseline—and determine what actions they’re ready, willing, and able to take
The opposite of assuming (often unconsciously) that clients are like you is, well, assuming nothing.
As best as you can, check your biases and assumptions at the door, and approach each client session with an open, curious mind.
Ask questions, such as:
“What inspired you—or pushed you—to come in today?”
And:
“Why is that goal meaningful to you?”
And:
“What skills do you have today that might help you achieve your goal? What skills do you feel you might be missing?”
Listen.
Withholding assumptions can be particularly difficult when clients share some obvious similarities with you. (Perhaps they’re also a single mom, or they’re also training for a triathlon, or they’re also a cancer survivor.)
But even when clients share similar experiences or goals, their biology, social context, personal history, and many other factors can make their “similar” experiences, in fact, totally different.
Coach Kate says in these cases, you can show that you relate to them, while also inviting them to describe their own experience. She suggests using the following question:
“I know what [insert shared experience] has been like for me, but what has [insert shared experience] been like for you?”
Once you have a clear picture of a client’s values, priorities, and reasons for change, you can assess which actions they’re ready, willing, and able to take. (Again, don’t make assumptions here. Just because you find meal prep quick and easy, doesn’t mean your client will.)
If you want to go through this exercise with your client on paper, use our Ready, Willing, and Able Worksheet.
Takeaway nugget:
Remember that clients:
- Aren’t always motivated by the same things as you (for example, they might care more about their next lab test results than how they look in a swimsuit)
- Don’t always enjoy—or hate—the same things (just because you love long sessions of steady state cardio, doesn’t mean they will… or vice versa)
- Don’t always share your values (as mentioned above, not all clients value health above all else; they may instead value pleasure, spontaneity, or something else)
Get to know your unique client, their specific goals, and what actions they can realistically execute (and maybe even get excited about).
Coaching mistake #3: Getting too attached to client results
This is, actually, very natural.
“There’s a reason we go into coaching. It’s because we care and we want to help clients. We want to see them succeed,” says Coach Kate.
But caring can be a double-edged sword.
“With our clients, we carefully decide on the habits and behaviors that need to occur… And then they walk off and either do the thing or don’t do the thing. That’s brutal.”
No matter how sound and foolproof your advice is, how well-thought out your plan, how much you care, ultimately, you have no control over whether a client executes it, and gets results.
Naturally, as a coach, you might feel frustrated, even heartbroken when clients don’t do what they say they’ll do, or when they’re not seeing the outcomes they were hoping to see.
However, according to Kate, this isn’t something coaches should try to avoid completely. It’s part of the job, and it’s often a sign that your work has meaning to you. (It’s a good thing.)
“However, I think there’s a point there where we can start caring more than the client themselves,” she says.
And that’s precisely where to draw to the line.
At PN, we often say that “care units” are the currency of coaching.
Care units are how much time, energy, attention, authenticity, and true “heart” you can bring to helping, serving, and caring about your clients.
Your client also has a certain amount of care units.
How much time, energy, attention, authenticity, and “heart” can they bring to their own change and growth projects?
(Most of the time, not that much. Which is totally normal.)
Our advice: Care one care unit less than your client does.
How do you do that? One approach…
Solution: Clearly separate client and coach responsibilities
So, how do we maintain an appropriate level of emotional investment—but also help clients stay on track?
“This is where I really like to get really clear on what my role is as a coach,” Coach Kate says.
“Because if you are very, very clear on what your role is as a coach, then you can sort of go through the list, and check in with yourself: ‘Did I show up? Did I follow up? Did I coach this person to the best of my ability?’”
For example, as a coach, it’s reasonable to be responsible for:
- Providing guidelines for how to reach out (to ask questions or book appointments) as well as setting expectations for your response times
- Weekly check-ins with clients via email, text, or phone, to assess progress or troubleshoot obstacles
- “Life-proofing” a program as much as possible, by proactively discussing obstacles that could arise in the future, and brainstorming realistic, flexible solutions
Meanwhile, the client is responsible for:
- Whether or not they respond to your check-ins
- Whether or not they actually DO the agreed upon fitness, nutrition, or lifestyle practices that are likely to get them to their goal
- How much they reveal during coaching sessions (for example, whether or not they tell you if they’re struggling with stress eating, or some other issue that makes it hard to stick to the plan)
Ideally, clearly delineating these responsibilities should happen early in the coaching relationship. Some coaches prefer to have an open discussion, while others have actual contracts that outline coach deliverables and client expectations.
This early communication can also be a way of vetting coach-client “fit.”
“When I’m having that initial conversation with a prospective client, I can ask, ‘What does accountability look like to you?’ If the client replies, ‘Well, I want you to text me every morning and night, and I want you to make sure I’ve done my workout, and also ship groceries to my house,’ then I will be the one to say, ‘I don’t think this is a good fit.’”
Coach Kate says this kind of early clarity can also prevent coach-client friction in the future.
Clear boundaries and expectations at the outset means clients are less likely to be disappointed if they assumed their coach was going to “take on” more, and coaches are less likely to burn out from shouldering more than they should.
It even protects the coach-client relationship in extreme (though not uncommon) situations such as when a client “ghosts” before a paid contract is over.
“When somebody doesn’t reply to me, I don’t take it personally. It’s not their job to reply, but it is my job to check in,” Coach Kate says.
“If I don’t hear back, I just check in on Monday, and then again on Monday. And again, and again, and again—trying all the contact methods they’ve provided me—until their coaching contract is over. If we get to that point, they’ll get an email from me saying, ‘Hey, I hope everything’s okay. My door is always open. I hope you’re doing well.’”
Takeaway nugget:
Make a list—either for your own reference, or to include in a contract that new clients have to sign—of the accountabilities you have as a coach.
(Hint: These are usually specific actions, like “Text, email, or phone once a week to check in” or “Host monthly virtual lectures on various nutrition topics for group clients.”)
Make sure to have a conversation about expectations and responsibilities with all clients, ideally before beginning to work together, or at least in the first session.
Bonus mistake: Forgetting to give yourself a pat on the back
It’s maybe not the most “coach-y” way to write an article: Point out a list of your mistakes, then hand you solutions to deal with them.
But if you’ve made the above “mistakes,” we want you to hear it from us:
We’re proud of you.
If you’ve gotten sidetracked by the above, it’s likely because you really care. And that’s never going to be a mistake; it’s a strength.
That said, although these “mistakes” are completely normal, and most coaches make them, they can limit your potential as a coach, and as a business.
And we want to see you succeed.
(If you liked this article and want to learn more, listen to the full episode of the Coaches Compass podcast, where the interview with Coach Kate Solovieva was originally conducted.)
If you’re a coach, or you want to be…
You can help people build sustainable nutrition and lifestyle habits that will significantly improve their physical and mental health—while you make a great living doing what you love. We’ll show you how.
If you’d like to learn more, consider the PN Level 1 Nutrition Coaching Certification. (You can enroll now at a big discount.)
The post Three mistakes health coaches make—and the immediately actionable solutions to fix them appeared first on Precision Nutrition.
Source: Health1
“I just bought a new BPA-free tupperware set.”
This comment, coming from my friend Anna, caught me off guard.
Anna’s a highly competent law professional. She’s a critical thinker and she fights in the heavyweight division when it comes to cutting through BS.
But the Anna I knew was falling into some painful traps that seemed to be bypassing her inner hawk-like skeptic.
She’s wanted to lose around 15lbs for some time now and came to me to share how stuck she was feeling in this goal.
She brought up an avenue she was exploring: the new BPA-free tupperware set.
“Interesting. What inspired you to focus on that?” I asked.
“Well, I’ve been reading about how microplastics in food containers can mess up our hormones and cause weight gain,” she said.
I squinted.
To backtrack, this is right after she told me how she’d been struggling to be consistent at the gym, had been relying on takeout too often, and had been sacrificing boring old sleep for adrenaline-inducing doom scrolling.
So I asked:
“What about trying to get more consistent with your workouts, or prepping more homemade meals during the week?”
And Anna said:
“Yeah, but I’ve tried that a thousand times. If it were that simple, it would have worked already.”
We’ve all done this before.
Ignored or delayed those hard-but-worthwhile habit changes in favor of some ultra-specific, niche magic bullet that’s supposed to “change everything.”
Spent hours of research on the ultimate, most optimal workout instead of devoting those hours to just doing the basic workout you already know how to do.
Waited to feel more inspired, motivated, or just less busy.
Why do we do this?
Buying new gear or a popular supplement feels like making progress.
Consuming YouTube videos or articles about stuff you can change feels like you’re doing something.
And waiting until the “right time” feels, well, right.
Except, nothing actually changes until we take real, consistent action.
We’re clever, us humans. And we’ve come up with lots of sneaky ways to avoid the basic, unsexy, difficult actions we need to take that actually drive change.
In this article, we’ll explore how to take an honest and compassionate look at why you might be distracting yourself from taking impactful action.
You’ll learn:
- What the most impactful health habits actually are
- Three common barriers to making sustainable progress
- A 4-step process you can apply to start taking positive, productive action
- How to keep yourself consistent—and achieve your goals
The stuff you know you should do (but probably aren’t doing consistently)
We all know what those basic, fundamental health habits are:
Exercising, ideally 30 minutes a day, putting in moderate-to-vigorous amounts of effort, with a mix of aerobic and resistance training.
Eating mostly nutritious, minimally-processed foods. If 80 percent of your diet comes from whole or minimally-processed foods, you’re doing an excellent job. (Translation: “Perfection” isn’t required; pizza can be part of a healthy diet.)
Eating enough protein to support muscle mass, appetite regulation, and body recomposition goals, if you have them. Aim for about 1.2 to 2.2 grams of protein per kilogram of body weight (for most people, this adds up to about 4-6 palm-sized portions of lean protein per day).
Prioritizing getting seven to eight hours of quality sleep. You can’t always control how well you sleep, but having some wind-down time before bed can help, as can waking up at the same time every day.
Avoiding or at least reducing excessive consumption of alcohol or drugs, including cigarettes. No fun, we know. But it’s for a good cause.
Easily, we could add stuff like prioritizing positive, nurturing social relationships, managing stress, and probably others, but just the above list is uncommonly met.
In fact, only six percent of Americans perform all five of the following basic health behaviors:1
- Meet physical activity recommendations
- Don’t smoke
- Consume alcohol in moderation (or not at all)
- Sleep at least seven hours
- Maintain a “normal” BMI
If you’re doing the math, that means close to 94 percent of Americans aren’t doing the basics.
Yet, these foundational behaviors also help us achieve a long list of common goals, whether that’s reaching a healthy weight, improving athletic ability, or just living a longer, healthier life.
So why do we struggle so much to do them?
Here are three common barriers we see among clients (and coaches!), plus potential solutions to overcome them.
By the way, ambivalence is normal.
That push-and-pull feeling you have when you think about making a change?
It has a name, and it’s called ambivalence.
Ambivalence describes the mix of feelings you have when you contemplate, say, waking up earlier so your mornings are less stressful, or cutting down on TV time.
We naturally and normally feel ambivalence about change—“I want this, and at the same time, that.”
(For example, wanting to eat healthier, and also wanting to have your favorite treats whenever you want without constraint.)
We also naturally and normally feel resistance towards change—“I want this, and at the same time, not.”
(For example, wanting to stop using your phone as a mindless distraction, but not wanting to deal with the anxiety you get whenever you’re left with your own thoughts.)
These contradictory emotions can seem frustrating, puzzling, or “illogical.” Yet, ambivalence and resistance are fundamental parts of the change process.
The higher the stakes of change, the more likely we are to feel a mix of strong and unexpected emotions, pushback, rebellion, angst, and other types of resistance and ambivalence.
Rather than signaling that the change is a wrong move, strong ambivalence and resistance tend to signal that this change matters to us.
In a sense, it’s good news.
It tells us we care.
Basics Barrier #1: You have ambition overload.
Maybe you’ve decided you want to be healthier. So you declare that, starting Monday, you’re going to exercise for an hour everyday and “eat clean” at every meal and sleep eight hours every night.
(Currently, you don’t have a regular exercise habit, don’t particularly like vegetables, and regularly stay up past midnight.)
Now, let’s be honest: You’re asking yourself to change a lot of stuff at once.
And the last time you created an elaborate plan for overhauling your life…
… Did it work?
Probably not.
(And that’s okay.)
When we feel frustrated or stuck in our current situation, making a plan filled with idealistic dreams can provide us temporary relief.
And our brain has several (normal) cognitive biases that prevent us from judging the future accurately.
We often think we’ll have more time, energy, attention, and motivation in the future than we really do.2 3 4 5
There’s a powerful, instantaneous comfort that comes with overloading our future self. (Because after all, we won’t start the plan until Monday.)
The problem with this is:
Big, complex plans often don’t fit into our already busy, complex lives.
We under-estimate how many smaller tasks are hidden in the bigger plans.
When we (almost inevitably) are unable to execute these ambitious goals, we blame ourselves, our personality traits, our “willpower” or “discipline,” and build a pitiable story about how we “struggle with consistency.” Or how living this way is “impossible”.
Then, sadly, we fulfill that prophecy.
Basics Barrier #2: You think only hardcore, “industry-secret,” or “cutting-edge” stuff works.
This barrier comes from the following common belief:
“If getting healthy just took eating, sleeping, and exercising moderately well, then everyone would be healthy.”
Because everyone knows they should eat their vegetables, get seven to eight hours of sleep per night, and stay active, right?
(We’d agree.)
But let’s go back to the previously mentioned statistic:
Only 6 percent of Americans are consistently performing the most basic health and fitness behaviors.
If we add on slightly more advanced—but still very basic—behaviors like eating five servings of fruits and vegetables every day, optimizing protein intake, and effectively managing stress, that number would shrink significantly.
So, the first thing is to believe that these simple behaviors work. Because they do. It’s just that most people (probably close to 99 percent of us) are not doing them all simultaneously and consistently.
The second thing is to accept that these simple behaviors are a little bit boring. Because they are. Part of the reason we’re attracted to new diets or “magical” supplements is because we just want something more interesting to try.
That’s especially true if we’ve already sort of tried the “eat more vegetables” thing and it didn’t “work” for us in the way we expected.
With something new and cutting-edge, there’s also the possibility of a new outcome, a new us.
And of course, that’s incredibly appealing.
Thing is, most hardcore, “industry secret,” or “cutting edge” tools and strategies are, respectively: unsustainable, inaccessible, or ineffective (or unproven).
They’ll take your effort, your time, and often your money, but without giving you a good return on your investment—all the while distracting you from the stuff that actually works.
Basics Barrier #3: You think your efforts (and your results) have to be perfect.
Another lie in the health and fitness industry is that you have to be “perfect” to maintain great health. You know, eat only organic salads and chia seeds, be able to run a marathon, and wake up at 5 am every day to meditate and write in your gratitude journal.
The truth is, perfection definitely isn’t required.
Depending on how you look at this, this could be a relief to hear, or a disappointment.
On the one hand, it’s nice to know that you don’t have to have it “all together” to be healthy—even above-average healthy.
On the other hand, many of us pursue better health with the belief that our optimal or even “perfect” self will one day, with the right plan or routine, be attainable.
But “perfect” health is an illusion.
Humans, even exceptionally healthy ones, get sick, get weird rashes, have digestive problems, need reading glasses, get into slumps, or just otherwise have a series of bad days.
None of us are “safe” from those life events, and accepting that can feel a little… vulnerable.
It’s much more comfortable to believe that if you just take this powdered algae supplement, or follow this specific morning routine, you’ll be immune to any kind of painful human experience.
The irony is, to achieve your realistic “best self,” you probably have to accommodate your “worst self” too. You know, the one who’d rather watch another episode of Love is Blind than work out, or eat a party-size bag of Doritos and call it dinner.
Because life happens.
Work gets busy.
Or your kid goes through a “phase.”
Or it’s pie season.
Any number of obstacles, distractions, and competing demands make it impossible for perfection to be maintained with any kind of consistency.
Which is why we need to let go of the illusion that a “perfect” self exists—the one who always has the energy, will, and option to make the ideal choice—and support what our real self wants and needs.
We’ve got four steps below to help you.
4 steps to start taking effective (and realistic) action
Now that we know what’s potentially getting in the way of taking productive action, here are four steps to get unstuck.
Step #1: Explore the why before the how.
Before you (or a client) start undertaking something you want to change, it’s helpful to understand your deeper motivations first.
Do a little investigating by asking questions like:
- What about this change is important to you?
- How serious or pressing is this for you?
- Why not continue doing what you’re already doing?
You can also go through one of our favorite motivation-mining exercises, The 5 Whys.
When you know why you want to change something, and you’re clear on the consequences of not taking action, you’ll be more likely to feel that deeper, more sustaining push to keep going, even when things get tough.
Step #2: Prioritize the most effective actions.
We can do all the things!! Really!! We just can’t do all the things… all at once.
Effective change means being able to realistically:
- Identify all the tasks, trade-offs, and commitments involved
- Prioritize what matters for the results you want
- Figure out what to do first
What are the essentials in relation to your goal? Regardless of all goals, they likely include a movement practice, a nutrition practice, and/or a recovery practice.
If you want some guidance on how to select the most effective action for your goal, check out our Skills, Practices, and Daily Actions Cheat Sheet.
Here’s how to use it:
Start with the domain you’re most interested in improving (such as “Nutrition” or “Stress”).
Then, get specific about what skill within that domain you’d like to improve (for example, “Eat well intuitively”), plus the practice that most appeals to you within that skill (say, “Eat to satisfied”).
Lastly, choose a daily action from the list of examples under your chosen practice. (For example, “Record hunger and fullness levels at the start and end of meals.”)
Once you choose your action, make it work for you by following step 3, below.
Step #3: Make sure you can take action, even on your worst day.
“I like to challenge a client to set a pathetic goal. If it’s so pathetic, then obviously you can do it, right?” says Kate Solovieva, PN Super Coach and Director of Community Engagement.
Sound inspiring?
Maybe not.
But if you’ve been struggling with consistency, it’s exactly where to start.
Ask yourself:
- What can I do on my absolutely worst day where everything goes wrong? How much time, effort, or enthusiasm will I realistically have?
Five minutes of walking? 10 push-ups? One extra portion of veggies? Three conscious deep breaths before every meal? Nothing is too small; it just has to be something.
Now you’ve got your floor.
Then ask yourself:
- What can I do on my best day, when I feel on top of the world and circumstances are on my side? How much time, effort, or enthusiasm will I realistically have?
One-hour of all-out effort at the gym? Two hours of meal prep that will feed you and your family for the next three days? A 45-minute guided meditation?
This is your ceiling.
Now that you’ve identified your “floor” and your “ceiling,” you’ve defined a flexible range of actions that can adapt to your fluctuating, unpredictable, real life.
But applying this range requires a paradigm shift:
Your health habits aren’t an “on” or “off” switch; they’re on a dial.
When life is sweet and smooth, you can turn your exercise, nutrition, and sleep dials way up—if you want. Bust through your PRs at the gym, eat all the arugula, meditate like a monk.
But if life gets nuts, you don’t have to switch off completely.
Just turn the dial down a little.
The below is a visual representation of how this might work for exercise, but you can apply this same thinking to your nutrition, sleep, stress management, or whatever you’re working on.
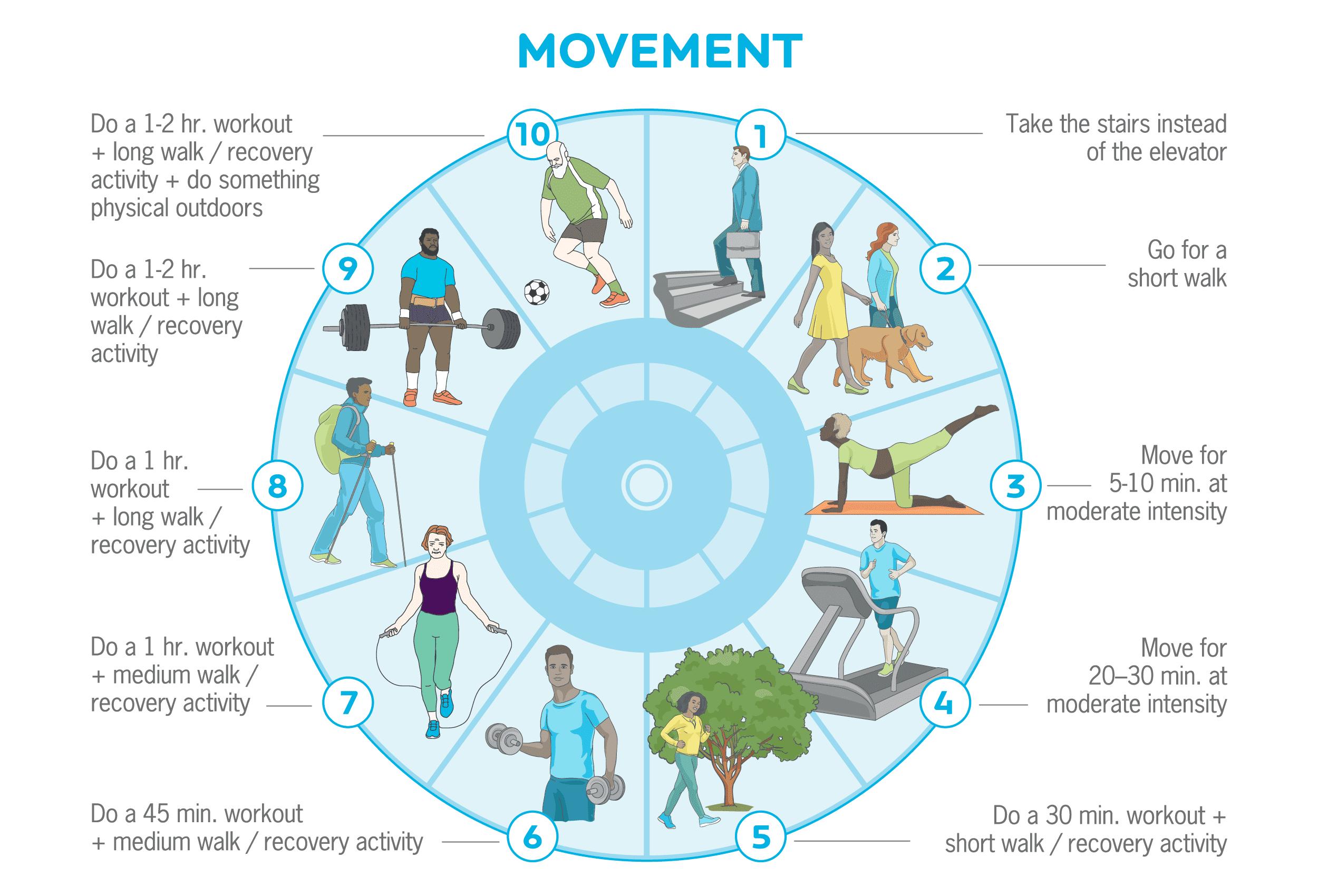
The important part: Even if you do your “floor” or “dial level 1” action—even if it’s for days on end—it still “counts.”
You still get the gold star.
Doing the bare minimum isn’t failing.
It’s succeeding, in the context of a real, messy, beautiful life.
Step #4: Create an ecosystem that supports you.
Health and fitness professionals often forget how different their lives are from their clients.
For example, many coaches work at gyms, enjoy being physically active, and hang out with other active people. Exercising regularly is almost easier to do than not do, because, as Coach Kate says, “they’ve built a life that makes that habit seamless.”
So if you want to make your health goals more likely, Coach Kate offers this advice:
“Build an ecosystem that makes failing nearly impossible.”
When they want to make a change, many people assume that good intentions and willpower will be enough to carry them through. (And when they fail, naturally, they blame themselves for being “bad” or “weak.”)
We often forget about the context and environment that shapes our behaviors—making certain actions more likely or less likely to occur.
A recent review from Nature Reviews Psychology ranked different behavior change strategies and found that access was the number one influencer of people’s behaviors. (People who lived in neighborhoods with affordable grocers close by ate better, just like people who had to drive a long distance to the closest gym were less likely to exercise.6)
Not everyone can change neighborhoods, but most people have some degree of control over their more immediate environments, and can leverage this power to shape desired behaviors.
One example is the “kitchen makeover,” where you make sure foods you want to eat are washed, prepped, and at the front of the fridge, ready to eat on a whim. Meanwhile, foods that don’t support your goals get tossed, or relegated to the highest cupboard. (When you need a stepladder from the basement to reach the cookies, you might find you eat them less.)
(If you want to try it out, check out our Kitchen Set-up Assessment worksheet.)
Think about the goal you want to achieve, and the behaviors that support it. Then, evaluate how you might make small changes to your environment by:
- Using a trigger: Sometimes called a “cue” or a “prompt,” a trigger is simply a reminder to do a desired action. For example, you might block the door of your home office with a kettlebell, reminding you that, every time you leave or enter the office, you have to do ten kettlebell swings. If you’re trying to cut down on mindless phone time, you can install an app that reminds you to shut things down after 20 minutes on social media.
- Decreasing “friction”: Supermarkets put candy next to the checkout, making it easy to slip that chocolate bar into your cart while you’re standing in line, likely bored and hungry. You can be equally sneaky about encouraging positive behaviors too, such as putting fruit on your counter, ready for a quick snack, or packing your gym bag the night before, so it’s ready to grab on your way out the door before you change your mind.
- Constraining available options: Whether it’s deleting time-sucking apps off your phone, removing foods you know you lose control around from your kitchen, or heck, creating a capsule wardrobe so you waste less time in the morning getting dressed, constraint can actually free up a lot of time, brain power, and energy.
Invest your energy building the ecosystem that nudges you to make desired actions the obvious choice. This requires a little more work on the front end, but the payoff will be greater for less overall work.
Embrace C+ effort.
If you’re a perfectionist, or a former straight-A student, that line hurt to read.
(Don’t worry. This C+ won’t result in your parents telling you that they’re disappointed.)
But what all of the above barriers and solutions have in common, is that they recognize and work with our inherent imperfection.
None of us is perfect, and expecting as much often results in failure (or at best, short bursts of success, followed by a crash).
Adopt an attitude of compassion and acceptance towards your human self—who’s most likely trying their hardest—and work with your vulnerabilities, instead of constantly expecting yourself to grit your teeth against them.
There will be times you’re getting “A’s” in fitness. That’s awesome. And you also don’t need to aim for C+. Just don’t think of yourself as a failure when you have to dial it down.
Living a healthy, meaningful life means constantly striving to do our best—while also allowing for flexibility, mistakes, and bad days (or seasons).
You’ll be surprised at how much better “good enough” is than nothing. Especially in the long run.
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
- Liu, Yong, Janet B. Croft, Anne G. Wheaton, Dafna Kanny, Timothy J. Cunningham, Hua Lu, Stephen Onufrak, Ann M. Malarcher, Kurt J. Greenlund, and Wayne H. Giles. 2016. Clustering of Five Health-Related Behaviors for Chronic Disease Prevention Among Adults, United States, 2013. Preventing Chronic Disease 13 (May): E70.
- Buehler R, Griffin D, Peetz J. Ch 1: The planning fallacy: cognitive, motivational, and social origins. In: Zanna MP, Olson JM, editors. Advances in Experimental Social Psychology. Academic Press; 2010. p. 1–62.
- Kruger J, Evans M. If you don’t want to be late, enumerate: Unpacking reduces the planning fallacy. J Exp Soc Psychol. 2004 Sep 1;40(5):586–98.
- Buehler R, Griffin D, Ross M. Exploring the “planning fallacy”: Why people underestimate their task completion times. J Pers Soc Psychol. 1994;67(3):366–81.
- Buehler R, Griffin D, Ross M. Inside the planning fallacy: The causes and consequences of optimistic time predictions. Heuristics and biases: The psychology of intuitive judgment. 2002;250–70.
- Albarracín D, Fayaz-Farkhad B, Granados Samayoa JA. Determinants of behaviour and their efficacy as targets of behavioural change interventions. Nature Reviews Psychology. 2024 May 3;1–16.
If you’re a coach, or you want to be…
You can help people build sustainable nutrition and lifestyle habits that will significantly improve their physical and mental health—while you make a great living doing what you love. We’ll show you how.
If you’d like to learn more, consider the PN Level 1 Nutrition Coaching Certification. (You can enroll now at a big discount.)
The post How to overcome barriers to better health appeared first on Precision Nutrition.
Source: Health1
When your eating plan stops working, it’s normal to just feel… stuck. But you can fix almost any diet problem with these 3 steps. (The first one might really surprise you).
++++
I’ve been working in the fitness and nutrition field for 25 years so I can say with certainty that every eating plan breaks down eventually. Kids come along, jobs get busy, family members get sick… LIFE happens.
It’s easy—too easy—to get lost.
But the exact nature of these nutrition breakdowns can vary. So, over the past few years, I’ve worked hard to come up with a formula that’ll fix almost any diet problem.
See, the nutrition “advice” you usually hear in the media and at the gym is often boiled down to buzzwords and slogans. You know the ones:
- “Just eat whole foods.”
- “Only eat food that your grandmother would recognize.”
- “Eat more fat and fewer carbs.”
- “If it doesn’t run, fly or swim–or it isn’t a green vegetable–don’t eat it.”
But when you’re a real human in the real world—or a professional helping one—slogans don’t get the job done.
Slogans lead to nutritional wheel spinning, frustration, and fat-loss plateaus—or even unwanted weight gain. They lead to:
Should I just quit already?
Why do I suck at this?
Will nutrition always come with frustration and failure?
It’s time to go beyond the clichés and discuss how to really help clients fix a broken diet and start eating better.
To share how we troubleshoot eating plans when they’ve “just stopped working” and you don’t know what else to try.
And, finally, to show you how to use these powerful and purposeful strategies to improve your own eating. Or to help others do the same.
These steps are proven to work—we’ve now tested them with over 70,000—and some of them may surprise you.
Step 1:
Remove nutritional deficiencies
When diets stop working, most people assume they need a complete overhaul right away.
I have to cut out sugar… and dairy… and carbs… and saturated fat.
Plus I have to eat more protein… more healthy fats… and more vegetables.
I have to start drinking lots of water too.
And exercise… maybe a 6 am boot camp… yeah.
Let’s call it the Mission Impossible approach.
Through lots of frustration and failure in my early career, I realized that the Mission Impossible approach isn’t just difficult; it’s misguided.
Because a complete overhaul rarely addresses what’s keeping most people from eating well in the first place.
The problem is: People feel bad. And it’s really hard to find the effort that’s required for a healthy diet when you feel bad most of the time.
Now, I call the root sources of feeling bad “limiting factors.” Limiting factors are the things that stand in the way of progress. They could be physical, mental, emotional.
Let’s focus on the physical first.
Physical limiting factors could be hormonal imbalances or sleep deprivation or too much lifestyle stress. However, a very common — and very commonly overlooked — limiting factor is actually dietary deficiency: not getting the right nutrients, in the right amounts, to look and feel your best.
Shocking percentages of the U.S. population are deficient in major nutrients.
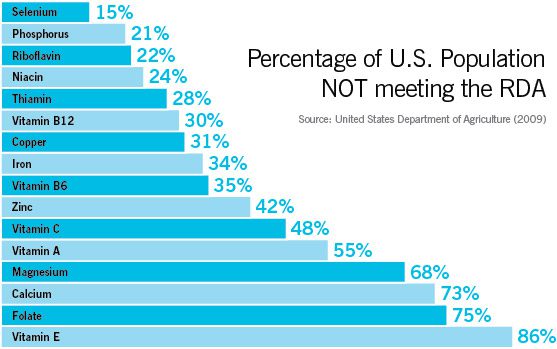
When it comes to deficiencies, a study published in the Journal of the International Society of Sports Nutrition backs this up: It’s really hard to get all the essential vitamins and minerals from food alone.
This study analyzed 70 athlete diets. Every single diet was deficient in at least three nutrients. And some diets were missing up to 15 nutrients! The most common deficiencies?
- iodine
- vitamin D
- zinc
- vitamin E
- calcium
Another study, also published in the Journal of the International Society of Sports Nutrition, showed that people following one of four popular diet plans (including Atkins, South Beach, and the DASH diet) were also very likely to be micronutrient deficient, particularly in six key micronutrients:
- vitamin B7
- vitamin D
- vitamin E
- chromium
- iodine
- molybdenum
Back when I was a graduate student at the University of Western Ontario, I set out to find the mythical “balanced diet.” I analyzed the intake of nearly 600 fourth-year exercise and nutrition undergraduate students.
Shockingly, less than 10 percent met the minimum standards for a “complete, balanced diet.” Like the other studies, these folks were missing such nutrients as:
- zinc
- magnesium
- vitamin D
- omega 3 fatty acids
- protein
In situations where populations are fed institutionally (i.e. prison inmates and school children) things can be even worse. But there’s hope.
Research in the British Journal of Psychiatry shows that providing fish oil and a multivitamin to prison inmates reduces aggressive and violent behavior by 35 percent and decreases antisocial behavior by 26 percent.
And a paper published in Nutrition Reviews shows that giving children fish oil and a multivitamin improves both their behavior and intelligence scores.
Bottom line: Dietary deficiencies are very common. Chances are, you’ve got one, no matter how good you think your diet is. At the same time, they’re not that hard to fix.
When you’re deficient in key nutrients, you feel bad.
As discussed above, optimized energy levels, appetite, strength, endurance, and mood all rely on getting enough essential nutrients.
That’s why you can eat clean, go Paleo, avoid meat, lower your carbs, or count calories–you can do “everything right” nutritionally–and still feel awful.
The most common deficiencies we see with new Precision Nutrition clients are:
- water (low-level dehydration)
- vitamins and minerals
- protein (particularly in women and in men with low appetites)
- essential fatty acids (95 percent of the population is deficient here)
The thing is, in the modern world, fixing a deficiency is pretty easy.
To find out if you (or your clients) are deficient in any area, there are a few options:
- Have a dietitian do a diet analysis.
- Record what you’re eating and enter it into an online nutritional calculator.
At Precision Nutrition, we like to make it even easier. As soon as clients begin with us, we do a quick survey of what they’re eating. Six questions tell us most of what we need to know. From there, we help them:
- eat more of the protein-rich foods they prefer;
- drink more hydrating fluids;
- supplement with essential fats (fish or algae oil); and/or
- eat more foods rich in the vitamins and minerals they need most.
As soon as they get these nutrients, they start getting results.
Our clients quickly start feeling better:
- Immediately energy levels go up.
- They feel more motivated.
- They lose fat and gain lean muscle.
- Their workouts become easier and better.
They start seeing the results that stopped when their diets “broke”.
In the end, the first step to fixing dietary problems is to identify and remove nutritional deficiencies.
Step 2:
Adjust food amount and food type
Once we’re getting all the raw materials necessary for proper functioning (i.e. essential nutrients) we can move on to bigger issues:
- food amount (what some call calorie intake); and
- food composition (which includes macronutrient breakdown).
In our coaching programs we help clients get away from using handbooks, websites, databases, spreadsheets, and math when planning meals.
You see, while we know that total food (calorie) intake matters, we’re not really fans of counting calories (for most people, most of the time).
To begin with, calorie counting does nothing to help us tune into our own powerful hunger and appetite cues. By learning how to listen to our own bodies, we have better long-term success in healthy eating.
(Of course, not everyone knows how to do this from the start. It takes a little coaching and some practice.)
Nor does calorie counting help us balance our health goals with our natural human enjoyment of food. In the short term, anyone can turn eating into a numerical and robotic exercise. But, in the long run, this strategy falls apart.
(Just ask anyone who “used to” count calories. You shouldn’t have a hard time finding them.)
There’s another problem with calorie counting: It’s just not all that accurate.
Because of imprecise labeling, lab errors, and differences in food quality and preparation, calorie counts recorded on food labels and websites–even those within the USDA’s nutrient databases–can be off by as much as 25 percent.
Then there’s the fact that human absorption is so wildly variable based on food preparation methods, and even the bacteria living inside your gut.
(If you really want to geek out with me, you can read this killer piece about how metabolism works. There are great sections on both the calories in and calories out sides of the energy balance equation.)
Bottom line: Even if you’re the world’s best calorie counter (and you can avoid the inevitable lifestyle problems associated with it) the math just doesn’t add up.
We teach most clients a different approach to calorie control.
The PN method for estimating portions requires nothing more than your own hand as the ultimate, portable measurement tool.
For example, men might begin by eating:
- 2 palms of protein dense foods at each meal;
- 2 fists of vegetables at each meal;
- 2 cupped handfuls of carb dense foods at most meals; and
- 2 thumbs of fat dense foods at most meals.
And women might begin by eating:
- 1 palm of protein dense foods at each meal;
- 1 fist of vegetables at each meal;
- 1 cupped handful of carb dense foods at most meals; and
- 1 thumb of fat dense foods at most meals.
First, we help clients see what this looks like. Like, in real life. On a plate.
Then, we adjust actual portion sizes up or down, depending on each person’s unique body and goals. For example:
- Men who want to add mass fast get an extra thumb of fat or an extra cupped handful of carbs per meal.
- But men who want to lose fat might scale down to 1 palm of protein, 1 thumb of fat, and 1 cupped handful of carbs per meal, eaten slowly and mindfully to 80 percent full.
Of course, just like any other form of nutrition planning–including detailed calorie counting–this is just a starting point.
You can’t know exactly how your body will respond in advance. So stay flexible and “steer dynamically.” Adjust your portions based on your hunger, fullness, overall activity level, and progress towards your goals.
(To get personalized hand-portion suggestions based on your eating pattern, goal, and several other variables, check out our free calculator.)
Food and macronutrient composition
Most people can simply eliminate nutrient deficiencies and get food portions and quality right, and stop there.
Small adjustments in those two areas—and nothing more—will make a huge difference in how 90% of folks look and feel. Simple. Easy.
However, for those who want to go further—because they have more advanced goals or because they’re already doing the first two and still struggling—let’s talk about food composition.
If you’re anything more than a casual observer of human beings, you might have noticed that—much like breeds of dogs—they come in different shapes and sizes. You’ll see everything from the giant wolfhound to the Chihuahua; everything from the slim and wiry whippet to the muscular bulldog to the rotund little Corgi.
Dog breeds also vary in their body composition, energy levels and metabolic rates… just like humans. Some people seem to be always fidgeting, always in motion; other people tend naturally to be more sedentary.
Different body type groups—aka “somatotypes”—typically include a few general characteristics:
- morphology and skeletal structure
- hormonal environment
- metabolism (including metabolic rate and how nutrients are processed)
If you specialize in a particular sport, especially at an elite level, you’ll often see that certain body types gravitate towards certain activities, or specific positions within sports.
(For a deeper dive into all of this, check out our article on body type eating.)
Step 3:
Fine tune the details
In the grand scheme of things, details like meal frequency, calorie/carb cycling, and workout nutrition–are just minor tweaks. Very minor tweaks. But let’s address them anyway.
Meal frequency
For years dietitians and nutritionists (myself included) thought that the best approach to splitting up your daily food intake was to eat small meals frequently throughout the day.
From early research we assumed that this would speed up the metabolism, help control the hormones insulin and cortisol, and help better manage the appetite. However we now know better.
All the latest research suggests that as long as we eat the right foods in the right amounts, meal frequency is a matter of personal preference.
You can eat lots of small meals each day (i.e. every few hours). Or you can eat a few big meals each day (i.e. with bigger time gaps between them).
Now, my advice is: Listen to your own body and apply the “how’s that workin’ for ya?” test.
If you’re covering all your other bases and your current meal frequency isn’t “workin’ for ya”, try switching it up. Experiment with fewer meals if you eat more frequently. And more meals if you eat less frequently.
Because either approach is valid, you’re free to find the approach that works best for you.
Calorie and carb cycling
Whether your goal is to lose weight, build muscle, see your abs, or get back in shape, carb and calorie cycling can make a real difference.
(Make sure deficiencies are eliminated, calories are controlled, and macronutrients are aligned appropriately–and that you’re doing all of this consistently before considering any of these fine-tuning strategies.)
While it may have a fancy name, carb cycling is simply eating more carbohydrates on some days–usually on high volume or high intensity days–and eating fewer carbohydrates on other days–usually low volume, low intensity, or off days.
We focus on carbohydrates (and not protein or fats) because carbs seem to influence body composition, how you look, and how you feel the most.
By changing carbohydrate and therefore calorie intake on particular days, we can keep fat loss going and metabolic rate humming along, without the ill effects of stringent calorie or carb restriction.
The carb and calorie cycling approach is pretty simple, and based on your activity.
- On the days you’re not lifting weights–or days you’re just doing low intensity or short duration exercise–eat a baseline diet of mostly protein, vegetables and healthy fats with minimal carbs.
- On the days you are lifting weights–or you’re doing longer duration high intensity exercise–add starchy carbs to your baseline diet.
And that’s pretty much it. No need to measure grams or count calories. Just follow a baseline diet on lower carb days. And add carbs on higher carb days.
Just remember this: Removing deficiencies, controlling calorie intake, and beginning eating for your body type–and doing this all consistently–must come first. If you haven’t done those first, this strategy usually backfires.
Workout nutrition
What should you have before, during, and after your workout?
If you’re training specifically for maximal muscle adaptation, and/or training with high volume and intensity (potentially multiple times every day), then eating an appropriate meal about 1-2 hours before and after training or competition may be important.
Also, for more advanced individuals, using a branched-chain amino acid drink (which is lower in carbs and calories), or a protein plus carbohydrate drink (which is higher in carbs and calories), during training can make a real difference in terms of adaptation and recovery.
However, if you’re exercising for general health and fitness–or simply to look and feel better–you should only consider the question of workout nutrition once you’ve:
- eliminated deficiencies;
- gotten your total food intake in check; and
- started eating right for your body type.
And—might I gently remind you—done all the above consistently. Yes, every day. Over and over and over.
What to do next:
Tips from Precision Nutrition
If you’re frustrated with an eating plan that’s not working–but aren’t sure what to do about it–hopefully this article has given you something new to consider and try.
1. Remove “limiting factors.”
If you feel bad, no diet is going to work for you. So start by rooting out and eliminating “limiting factors”. This includes addressing any sleep problems and talking to your doctor if you feel there may be a hormone imbalance.
But the most common—and commonly overlooked—problem is nutritional deficiency. And the easiest way to wipe it out is by:
- eating more protein-rich foods;
- drinking more hydrating fluids;
- supplementing with essential fats (fish or algae oil); and/or
- eating more foods rich in the vitamins and minerals you need most.
2. Calibrate food amount and type
Make sure you (or your clients) are eating the right kind and amount of food.
Use our free calculator to get personalized hand-portion recommendations. (And feel free to print out our infographic on portions for your clients/patients.)
From there, adjust portions based on appetite, meal frequency, activity level, weight goals, and results.
Then, if you feel the diet could be further tailored, consider adjusting portions for your body type.
3. Be consistent.
With these strategies, you should get results relatively quickly in most cases. But not overnight, and not if you’re inconsistent.
The key to staying consistent while fixing a broken diet: accountability. That could mean a food journal, a trainer, a trusted partner or friend, or an experienced nutrition coach.
If you’re a coach, or you want to be…
Learning how to coach clients, patients, friends, or family members through healthy eating and lifestyle changes—even when life is crazy-busy (read: always)—is both an art and a science.
If you’d like to learn more about both, consider the Precision Nutrition Level 1 Certification. The next group kicks off shortly.
What’s it all about?
The Precision Nutrition Level 1 Certification is the world’s most respected nutrition education program. It gives you the knowledge, systems, and tools you need to really understand how food influences a person’s health and fitness. Plus the ability to turn that knowledge into a thriving coaching practice.
Developed over 15 years, and proven with over 100,000 clients and patients, the Level 1 curriculum stands alone as the authority on the science of nutrition and the art of coaching.
Whether you’re already mid-career, or just starting out, the Level 1 Certification is your springboard to a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results.
[Of course, if you’re already a student or graduate of the Level 1 Certification, check out our Level 2 Certification Master Class. It’s an exclusive, year-long mentorship designed for elite professionals looking to master the art of coaching and be part of the top 1% of health and fitness coaches in the world.]
Interested? Add your name to the presale list. You’ll save up to 30% and secure your spot 24 hours before everyone else.
We’ll be opening up spots in our next Precision Nutrition Level 1 Certification on Wednesday, April 8th, 2020.
If you want to find out more, we’ve set up the following presale list, which gives you two advantages.
- Pay less than everyone else. We like to reward people who are eager to boost their credentials and are ready to commit to getting the education they need. So we’re offering a discount of up to 30% off the general price when you sign up for the presale list.
- Sign up 24 hours before the general public and increase your chances of getting a spot. We only open the certification program twice per year. Due to high demand, spots in the program are limited and have historically sold out in a matter of hours. But when you sign up for the presale list, we’ll give you the opportunity to register a full 24 hours before anyone else.
If you’re ready for a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results… this is your chance to see what the world’s top professional nutrition coaching system can do for you.
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
Carlton JB. Prevalence of micronutrient deficiency in popular diet plans. J Int Soc Sports Nutr. 2010; 7:24.
Frensham LJ, Bryan J, Parletta N. Influences of micronutrient and omega-3 fatty acid supplementation on cognition, learning, and behavior: methodological considerations and implications for children and adolescents in developed societies. Nutr Rev. 2012. 70:10.
Gesch C Bernard, Hammond Sean M, Hampson Sarah E, Eves Anita, Crowder Martin J. Influence of supplementary vitamins, minerals and essential fatty acids on the antisocial behavior of young adult prisoners. Br. J Psychiatry. 2002. 181:1.
Misner B. Food alone may not provide sufficient micronutrients for preventing deficiency. J Int Soc Sports Nutr. 2006;3(1):51–55.
The post The 3 steps I teach trainers and health coaches to help fix any diet problem. appeared first on Precision Nutrition.
Source: Health1
“I’ll get back to the gym as soon as…
… work slows down.
… the kids are back in school.
… we’re done working on the house.”
Most of us can come up with any number of worthy-feeling justifications for taking a “breather” from our health and fitness efforts.
But often, it all comes down to the one essential reason:
“Life is busy and stressful. I need to press ‘pause’ until things slow down and are less crazy.”
Except… things never really slow down permanently.
So we get stuck in an endless cycle: Giving health and fitness our all, then inevitably giving up when there’s something standing in the way of getting to the gym, eating well, or heading to bed at a reasonable hour.
With that all-or-nothing approach, we never really get anywhere.
But what if there were a way to keep you (or your clients) making progress—even during the busiest days, weeks, and months?
Introducing the “dial” method: an incredibly simple tool for scaling your health habits up and down based on what’s going on in your life.
Instead of “all or nothing,” this method helps you strive for “always something.”
The best part? You’ll never have to worry about “falling off the fitness wagon” again.

Download this infographic for your tablet or printer to help you stick with your healthy habits (or, if you’re a coach, to help your clients).
And for an even more in-depth look at this topic, check out our accompanying article, Why the “pause-button mentality” is ruining your health and fitness.
++++
If you’re a coach, or you want to be…
Learning how to coach clients, patients, friends, or family members through healthy eating and lifestyle changes—even when life is crazy-busy (read: always)—is both an art and a science.
If you’d like to learn more about both, consider the Precision Nutrition Level 1 Certification. The next group kicks off shortly.
What’s it all about?
The Precision Nutrition Level 1 Certification is the world’s most respected nutrition education program. It gives you the knowledge, systems, and tools you need to really understand how food influences a person’s health and fitness. Plus the ability to turn that knowledge into a thriving coaching practice.
Developed over 15 years, and proven with over 100,000 clients and patients, the Level 1 curriculum stands alone as the authority on the science of nutrition and the art of coaching.
Whether you’re already mid-career, or just starting out, the Level 1 Certification is your springboard to a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results.
[Of course, if you’re already a student or graduate of the Level 1 Certification, check out our Level 2 Certification Master Class. It’s an exclusive, year-long mentorship designed for elite professionals looking to master the art of coaching and be part of the top 1% of health and fitness coaches in the world.]
Interested? Add your name to the presale list. You’ll save up to 30% and secure your spot 24 hours before everyone else.
We’ll be opening up spots in our next Precision Nutrition Level 1 Certification on Wednesday, April 8th, 2020.
If you want to find out more, we’ve set up the following presale list, which gives you two advantages.
- Pay less than everyone else. We like to reward people who are eager to boost their credentials and are ready to commit to getting the education they need. So we’re offering a discount of up to 30% off the general price when you sign up for the presale list.
- Sign up 24 hours before the general public and increase your chances of getting a spot. We only open the certification program twice per year. Due to high demand, spots in the program are limited and have historically sold out in a matter of hours. But when you sign up for the presale list, we’ll give you the opportunity to register a full 24 hours before anyone else.
If you’re ready for a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results… this is your chance to see what the world’s top professional nutrition coaching system can do for you.
The post How to stop pressing “pause” on your health and fitness efforts. appeared first on Precision Nutrition.
Source: Health1
There’s a lot of discussion in the fitness industry about whether crash dieting can cause metabolic damage. In this article, we’ll take on this interesting topic and separate fact from fiction. We’ll also teach you exactly why crash diets might be linked to struggling to maintain your weight in the future.
++++
Despite working out consistently and intensely, plus eating carefully, you’re not losing weight (or not losing it as fast as you’d like or expect).
Or you were losing weight consistently… until recently. Now you’re stuck—even though you’re working as hard as ever.
Or when you were younger, you were super fit. Maybe you did fitness competitions. Maybe you did some crash diets. But now, even when you put in the same effort, you just can’t seem to get as lean.
“Is my metabolism damaged?”
Precision Nutrition Coaching clients ask us this question all the time.
(If you’re a health, fitness or wellness professional, you’ve probably heard it from your clients or patients too.)
Can months or years of dieting do some kind of long-term harm to the way the human body processes food?
Not exactly.
But gaining and losing fat can change the way your brain regulates your body weight.
To understand this answer let’s explore how human metabolism actually works. Then we’ll talk about whether the metabolism can actually be damaged.
Note: This post delves into the science of energy balance, thermodynamics, and metabolic regulation. If you love learning this stuff, feel free to dig in.
If, on the other hand, you’re simply looking for solid, research-backed advice on how to lose fat and break weight-loss plateaus, feel free to skip to the summary at the end.
Energy balance: The laws of physics still apply.
You need a certain amount of energy (in the form of calories) to stay alive, as well as to move around. You can get this energy from food, or you can retrieve it from stored energy (e.g. your fat tissue).
In theory:
- If you eat less energy than you expend, you should lose weight.
- If you do the opposite (i.e. eat more energy than you expend), you should gain weight.
In other words:

*We use the term “body stores” deliberately as it represents the tissues available for breakdown (fat, muscle, organ, bone, etc) and excludes water (which can change body weight independently of energy balance).
This relationship between ‘energy in’ and ‘energy out’ is called the Energy Balance Equation, and it’s the most commonly accepted model for calculating a person’s energy balance and how much weight they’ll lose or gain over time.
While the Energy Balance Equation determines body weight, it doesn’t tell us much about body composition, which is influenced by things like sex hormone levels, macronutrient intake (especially protein), exercise style / frequency / intensity, age, medication use, genetic predisposition, and more.
Understandably, people get really frustrated and confused with the Energy Balance Equation when the numbers don’t seem to add up, or their results don’t match their expectations. (This is a good lesson, by the way, about the importance of adjusting your expectations to match observable reality.)
And it’s a fair frustration. Most of the time, the numbers don’t add up.
Importantly:
This mismatch between expectations versus reality is not because the Energy Balance Equation is wrong, or a myth. Nobody’s body defies the laws of physics, even though it seems like that sometimes.
It’s because the equation is more complicated than it sounds.
Many factors affect the Energy Balance Equation; they aren’t mutually exclusive. What you do to ‘energy in’ affects what happens to ‘energy out’. And vice versa.
“Eat less, move more” is a good start. (Most of us could probably benefit from eating a little less and getting a little more daily activity.)
But that advice alone isn’t enough. It doesn’t take all of the complex, intersecting factors into account.
Let’s take a look at some of these factors, starting with the ‘energy in’ part of the equation.
‘Energy in’ is trickier than you think.
Reason 1: The number of calories in a meal likely doesn’t match the number of calories on the labels or menu.
This might sound hard to believe, but it’s true… the way companies (and even the government) come up with calorie and nutrient estimates is incredibly complex, rather imprecise, and centuries-old. As a result, food labels can be off by as much as 20-25 percent.
And even if those food labels were correct:
Reason 2: The amount of energy a food contains in the form of calories is not necessarily the amount of energy we absorb, store, and/or use.
Remember that the food we eat has to be digested and processed by our unique bodies. The innumerable steps involved in digestion, processing, absorption, storage, and use—as well as our own individual physiological makeup—can all change the energy balance game.
So, for instance:
- We absorb less energy from minimally processed carbohydrates, and fats, because they’re harder to digest.
- We absorb more energy from highly processed carbohydrates and fats, because they’re easier to digest. (Think of it this way: The more “processed” a food is, the more digestion work is already done for you.)
For example, research has shown that we absorb more fat from peanut butter than from whole peanuts. The researchers found that almost 38 percent of the fat in peanuts was excreted in the stool, rather than absorbed by the body. Whereas seemingly all of the fat in the peanut butter was absorbed.
In addition:
- We often absorb more energy from foods that are cooked (and/or chopped, soaked, blended) because those processes break down plant and animal cells, increasing their bioavailability.
When eating raw starchy foods (like sweet potatoes), we absorb very few of the calories. After cooking, however, the starches are much more available to us, tripling the number of calories absorbed.
Interestingly, allowing starchy foods to then cool before eating them decreases the amount of calories we can extract from them again. (This is mostly due to the formation of resistant starches).
Finally:
- We may absorb more or less energy depending on the types of bacteria in our gut.
Some people have larger populations of a Bacteroidetes (a species of bacteria), which are better at extracting calories from tough plant cell walls than other bacteria species.
Here’s an interesting example of this whole process at work. Recently, USDA researchers asked test subjects to consume 45 grams (about 1 ½ servings) of walnuts daily for three weeks.
What they found was that, on average, people only absorbed 146 of the 185 calories in the nuts. That’s 79 percent of the calorie content on the label.
In similar research, people also absorbed only 80 percent of the calories in almonds, and 95 percent of the calories in pistachios.
Beyond the average, there were individual differences: Some people absorbed more of the energy in the nuts, while some absorbed less (likely due to the differing populations of bacteria in their large intestines).
In the end, by eating a diet rich in whole, minimally processed foods, the number of calories you absorb can be significantly less than what you expect. Plus they require more calories to digest.
Conversely, you will absorb more calories by eating lots of highly processed foods, plus burn fewer calories in the digestive process. (In addition, highly processed foods are less filling, more energy dense, and more likely to cause overeating.)
Since the number of calories someone thinks they’re consuming could be off by 25 percent (or more), their carefully curated daily intake of 1,600 calories could really be 1,200… or 2,000.
This means:

As you can see, there’s a big margin of error for energy input, even if you’re a conscientious calorie counter. This doesn’t invalidate the Energy Balance Equation. It just means that if you want an accurate calculation, you probably have to live in a fancy metabolic lab.
For most people, it’s not worth the effort (that’s one reason why Precision Nutrition moved to a hand-based measuring model for portions).
‘Energy out’ varies a lot from person to person.
‘Energy out’—again, energy burned through daily metabolism and moving you around—is a dynamic, always-changing variable.
There are four key parts to this complex system:
1. Resting metabolic rate (RMR)
RMR is the number of calories you burn each day at rest, just to breathe, think, and live. This represents roughly 60 percent of your ‘energy out’ and depends on weight, body composition, sex, age, genetic predisposition, and possibly (again) the bacterial population of your gut.
A bigger body, in general, has a higher RMR.
For instance:
- A 150-pound man might have an RMR of 1583 calories a day.
- A 200-pound man might have an RMR of 1905 calories.
- A 250-pound man might have an RMR of 2164 calories.
Crucially, RMR varies up to 15 percent from person to person. If you’re that 200-pound guy with an RMR of 1905 calories, another guy just like you on the next treadmill might burn 286 more (or fewer) calories each day with no more (or less) effort.
2. Thermic effect of eating (TEE)
This may surprise you, but it takes energy to digest food. Digestion is an active metabolic process. (Ever had the “meat sweats” or felt hot after a big meal, especially one with lots of protein? That’s TEE.)
TEE is the number of calories you burn by eating, digesting, and processing your food. This represents roughly 5-10 percent of your ‘energy out’.
In general, you’ll burn more calories in your effort to digest and absorb protein (20-30 percent of its calories) and carbs (5-6 percent) than you do fats (3 percent).
And as noted before, you’ll burn more calories digesting minimally processed whole foods compared to highly processed foods.
3. Physical activity (PA)
PA is the calories you burn from purposeful exercise, such as walking, running, going to the gym, gardening, riding a bike, etc.
Obviously, how much energy you expend through PA will change depending on how much you intentionally move around.
4. Non-exercise activity thermogenesis (NEAT)
NEAT is the calories you burn through fidgeting, staying upright, and all other physical activities except purposeful exercise. This, too, varies from person to person and day to day.
This means:

Each of these is highly variable. Which means the ‘energy out’ side of the equation may be just as hard to pin down as the “energy in” side.
So, while the Energy Balance Equation sounds simple in principle, all these variables make it hard to know or control exactly how much energy you’re taking in, absorbing, burning, and storing.
Here’s the entire equation:

When you try to outsmart your body and it outsmarts you back.
Even if all the variables in the final equation above were static, the Energy Balance Equation would be complicated enough. But things get crazy when you consider that altering any one of the variables causes adjustments in other, seemingly unrelated variables.
This is a good thing, of course. Our human metabolisms evolved to keep us alive and functioning when food was scarce. One consequence:
When ‘energy in’ goes down, ‘energy out’ goes down to match it. (You burn fewer calories in response to eating less).
Not in everybody. And not perfectly. But that’s how the system is supposed to work. That’s how our bodies avoid unwanted weight loss and starvation. It’s how humans have survived for 2 million years. The body fights to maintain homeostasis.
Likewise, when ‘energy in’ goes up, ‘energy out’ tends to go up too. (You burn more calories in response to eating more).
To illustrate this point, here’s how your body tries to keep your weight steady when you take in less energy and start to lose weight*.
- Thermic effect of eating goes down because you’re eating less.
- Resting metabolic rate goes down because you weigh less.
- Calories burned through Physical activity go down since you weigh less.
- Non-exercise activity thermogenesis goes down as you eat less.
- Calories not absorbed goes down and you absorb more of what you eat.
*This response is particularly modest at first. But the adaptation really ramps up as you lose more weight. (Or if you’re starting out lean and trying to get super-lean).
Check out what this looks like:
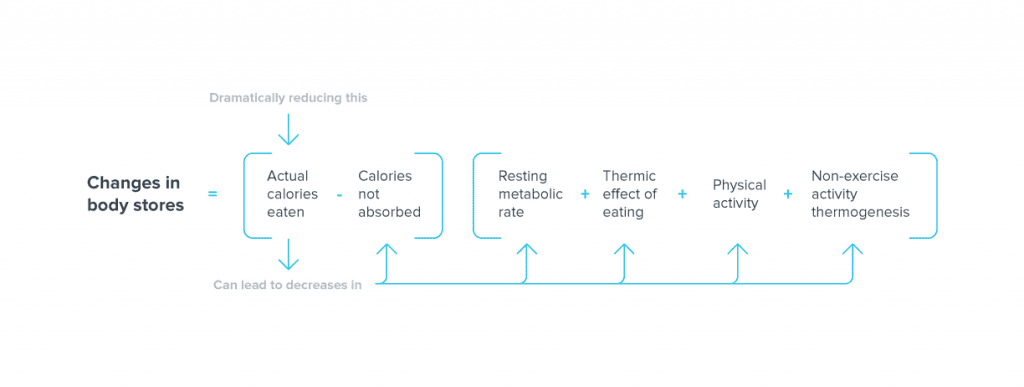 In addition to these tangible effects on the equation, reducing actual calories eaten also causes hunger signals to increase, causing us to crave (and maybe eat) more.
In addition to these tangible effects on the equation, reducing actual calories eaten also causes hunger signals to increase, causing us to crave (and maybe eat) more.
The net effect leads to a much lower rate of weight loss than you might expect. In some cases, it could even lead to weight re-gain.
To add insult to injury, a rise in cortisol from the stress of dieting can cause our bodies to hold onto more water, making us feel “softer” and “less lean” than we actually are.
Interestingly, this is just one example of the amazing and robust response to trying to manipulate one variable (in this case, actual calories eaten). There are similar responses when trying to manipulate each of the other variables in the equation.
For example, research suggests that increasing physical activity above a certain threshold (by exercising more) can trigger:
- Increased appetite and more actual calories eaten
- Decreased calories not absorbed as we absorb more of what we eat
- Decreased RMR
- Decreased NEAT
In this case, here’s what the equation would look like:
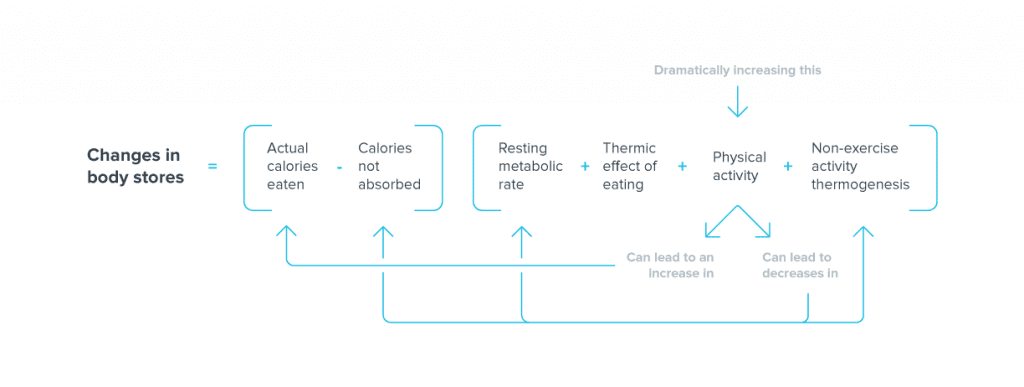 In the end, these are just two of the many examples we could share. The point is that metabolism is much more complicated (and interdependent) than most people realize.
In the end, these are just two of the many examples we could share. The point is that metabolism is much more complicated (and interdependent) than most people realize.
Therefore, trying “what used to work” for you, or relying on calorie counting, often won’t get you the results you want. As your energy balance evolves, so must your strategies for losing fat or maintaining your weight.
Understanding energy balance means setting better expectations about body change.
It’s important to note that if you have lots of body fat to lose, many of these adaptations (i.e. lowered RMR, PA, NEAT, etc) don’t happen right away. But, as you become leaner, this “adaptive thermogenesis” kicks in.
It’s also important to know that how your metabolism reacts to changes in energy balance will be unique to you.
How much you can lose or gain will depend on your age, your genetic makeup, your biological sex, if you’ve had relatively more or less body fat and for how long, what medications you’re taking, the makeup of your microbiome… and probably a whole lot of factors we don’t even know about yet.
But let’s try to simulate how this could work.
Scientists at the National Institutes of Health have studied the data from people who have lost weight, and created a mathematical model that represents how weight and fat loss actually happens in the real world.
We can play with it, using the Precision Nutrition Weight Loss Calculator.
Let’s start with a 40-year-old male, with a starting weight of 235 lb and a height of 5’10”. We’ll call him Frank.
Frank works a desk job, and is only lightly active outside of work. This calculates that he needs 2,976 calories of energy per day to maintain his current weight.
By knocking off 500 calories per day, his intake drops to 2,476 calories daily. And he doesn’t plan on changing his physical activity.
Now, you’ve probably heard somewhere that a pound is equivalent to 3,500 calories, which means that if we take away those 500 calories from Frank every day, he should lose 1 pound per week (500 x 7 days = 3500 calories).
He should end up at 183 lb after one year of consistently eating 500 fewer calories every day. (According to this math, then, he would weigh 0 lb within 5 years, which should raise some red flags.)
But we know it doesn’t exactly work this way in real life.
At the end of a year, Frank gets on the scale. He’s 205 lb.
What the hell?
That’s 22 pounds more than I should be!
Frank rages to his wife Maria, who smiles knowingly. She’s 40 too, and has been trying to lose weight since having two kids in her mid-30s.
Tell me about it, she says. I’ve lost and gained the same 10 pounds over and over, even though I’ve been exercising and eating pretty healthy.
Then they both think:
Maybe I should try that juice cleanse after all. My body is obviously broken.
Nope, nobody is broken. Don’t hit that juice cleanse just yet.
Instead, Frank and Maria could both benefit from a clear understanding of how weight loss actually works. Then they can set appropriate behavior goals, and have realistic expectations for their progress.
(Postscript: Frank and Maria decide against the juice fast and enroll in Precision Nutrition Coaching. At the end of a year, Maria “only” lost a total of 7 lb, but has gained 5 lb of muscle [which means she’s lost 12 lb of fat]. Her firm arms and glowing skin are the envy of the other moms. Frank is down to a fit 185 lb and trying to figure out how to convince Maria that he should buy a mountain bike.)
So, does dieting damage the metabolism?
Despite what you may have heard:
No, losing weight doesn’t “damage” your metabolism.
But because of the adaptations your body undergoes in response to fat loss (to prevent that fat loss, in fact), ‘energy out’ for those who have lost significant weight will always be lower than for people who were always lean.
Rather:
Losing weight, and keeping it off, is accompanied by adaptive metabolic, neuroendocrine, autonomic, and other changes.
These changes mean that we expend less energy—around 5-10 percent less (or up to 15 percent less at extreme levels) than what would be predicted based on just weighing less.
Unfortunately, because of this adaptive response, someone who has dieted down will often require 5-15 percent fewer calories per day to maintain the weight and physical activity level than someone who has always been that weight.
(Or even less, potentially, because as we learned in the very beginning, the RMR of people of the exact same age/weight/etc. can still vary by up to another 15 percent.)
This means someone who was never overweight might need 2,500 calories to maintain their weight, while someone who had to diet down to that weight may need only 2,125-2,375 calories to hold steady.
We don’t know how long this lowered energy expenditure lasts. Studies have shown that it can hang around for up to 7 years after weight loss (or more; 7 years is as far as it’s been studied). This likely means it’s permanent, or at least persistent.
This is extra relevant for people who have repeatedly dieted, or for fitness competitors who may repeatedly fluctuate between being extremely lean and being overweight in the off-season.
I don’t have data to back this up (to my knowledge no one has studied it), but adaptive thermogenesis seems to react more strongly or more rapidly with each successive yo-yo of extreme body fat fluctuations.
All of this explains why some people can feel like they’ve “damaged” their metabolism through repeated dieting. (And why some experts suggest “metabolic damage” is a real thing.)
But nothing really has been “damaged”.
Instead, their bodies have just become predictably more sensitive to various hormones and neurotransmitters. Their metabolic rates are understandably lower than predicted by various laboratory equations.
So, where does this leave us?
Even folks whose bodies resist fat loss or muscle gain can accomplish these goals.
All physiological changes—including weight loss or gain, fat loss or gain, and muscle loss or gain—require different efforts and amounts of time for different people.
But even if your body does resist weight loss, you can still lose fat, gain muscle, and dramatically change your body.
Our Precision Nutrition Coaching men’s and women’s Finalist Halls of Fame are clear evidence of that.
What to do next:
Some tips from Precision Nutrition.
The physiology of weight loss is complicated, but the best strategies for losing fat and keeping it off don’t have to be.
1. Eat plenty of protein.
Protein is essential when trying to losing weight / fat for a few reasons.
- Protein helps you keep that all-important lean body mass (which includes connective tissues, organs, and bone as well as muscle).
- Protein significantly increases satiety, which means you feel fuller despite eating less. (And eating more protein often causes people to eat less overall.)
- Just by eating more protein you burn more calories, because of the increased thermic effect of eating.
For example, if you’re eating 2,500 calories daily, 15 percent from protein, 50 percent from carbs, and 35 percent from fats (roughly average for US adults), you’re burning approximately 185 calories per day through digestion.
Maintain your total calorie intake but increase protein to 30 percent, drop carbs to 40 percent, and whittle fat to 30 percent, and your TEE goes up to roughly 265 calories per day.
- For most active men: 6-8 palm-sized servings of protein per day.
- For most active women: 4-6 palm-sized servings per day.
For a complete guide to using your hand to measure portions, check out our Calorie Control Guide infographic.
2. Eat a wide variety of fruits, vegetables, quality carbs, and healthy fats.
Vegetables are loaded with vitamins, minerals, phytonutrients, water, and fiber to help you fill up during meals, stay full between meals, keep you healthy, and recover from your workouts.
- We recommend 6-8 fist-sized servings per day for most active men.
- And 4-6 fist-sized servings per day for most active women.
The carbs will fuel training, boost leptin (a super important hormone), keep up sex hormones, and prevent feelings of deprivation.
And the fats also keep up sex hormones, boost the immune system, suppress excess inflammation, and make food taste really good.
- For most active men, this would be 6-8 handfuls of quality carbs, and 6-8 thumbs of healthy fats per day.
- For most active women, 4-6 handfuls of quality carbs and 4-6 thumbs of healthy fats per day.
For a complete guide to using your hand to measure portions, check out our Calorie Control Guide infographic.
3. Adjust your intake as you plateau, or to prevent plateaus.
As your weight loss progresses, you will need to lower your calorie intake further to continue to progress, as your smaller body will burn fewer calories, and your body is adapting to your diet.
Be ready, willing, and able to adjust portion amounts by removing 1-2 handfuls of carbs and/or 1-2 thumbs of fats from your daily intake. Then reassess and continue to adjust as needed.
However, one study found that weight loss plateaus have less to do with metabolic adaptations and more to do with “an intermittent lack of diet adherence”. In other words, not actually sticking to a nutrition plan consistently.
Research shows that we usually think we’re eating less and exercising more than we truly are. So do an objective review of your actual energy in and out before assuming your body is blocking your efforts.
4. Understand that this is complex.
So many things influence what, why, and when we choose to eat.
Too often, eating and body size / fatness are blamed on lack of knowledge, lack of willpower/discipline, or laziness. In reality, food intake and body composition are governed by a mix of physiological, biological, psychological, social, economical, and lifestyle influences, along with individual knowledge or beliefs.
One of the simplest ways to make your decision processes easier is to create an environment that encourages good food choices and discourages poor ones. This can mean making changes to your daily routine, who you spend time with, where you spend time, and what food is readily available to you.
But remember that weight loss can and should be relatively slow, so aim to lose about 0.5-1 percent of your body weight per week.
This helps to maintain muscle mass and minimize the adaptive metabolic responses to a lower calorie intake and resulting weight loss. Faster weight loss tends to result in more muscle loss without extra fat loss, as well as a larger adaptive response.
5. Cycle calories and carbs.*
For folks who are trying to get quite lean, at some point you can’t just rely on linear dieting to get you there. By strategically cycling calories and carbs, you can help to limit how much the metabolism-regulating hormone leptin drops (or temporarily boost it back up) – attenuating the adaptive and hunger response.
*Note: This is a higher-level strategy for fitness competitors and elite athletes who need to get very lean (i.e. ~6-9 percent body fat for men, and ~16-19 percent for women). It’s not something for the average person.
6. Refeed periodically.**
When getting to extreme levels of leanness, even strategic calorie and carb cycling might not be enough. So take out the big guns, and employ some periodic re-feeds to temporarily boost leptin and insulin and keep fat loss going.
**Note: This is a higher-level strategy for fitness competitors and elite athletes who need to get very lean (i.e. <6 percent body fat for men, and <16 percent for women).
7. Do a mixture of resistance, cardiovascular, and recovery activity.
Resistance training helps you maintain vital muscle mass, burn calories, and improve glucose tolerance. Cardiovascular exercise improves the health of your cardiovascular system, helps you expend energy, and can improve recovery.
Recovery work (e.g. foam rolling, walking, yoga) helps you maintain consistency and intensity with resistance and cardio training, making them more effective. And it helps to decrease stress (lowering cortisol), which also helps you lose body fat and keep it off.
Aim for 3-5 hours per week of purposeful activity.
8. Find ways to increase NEAT.
Even small increases in activity can account for hundreds of daily calories, and therefore make a big difference in fat loss efforts.
Some ideas: Get a stand-up desk or a treadmill desk; fidget; pace while on the phone; take the stairs; park your car farther away from where you’re going.
9. Develop a solid nightly sleep routine and manage your stress.
Sleep is just as important to your success as nutrition and activity levels. Don’t pretend that you can get by with less. It simply isn’t true.
Often, when people lower their stress, they lose a lot of body water. Then they also notice that they may have lost fat too. (Plus, they may discover that chronic inflammation goes down—another win.)
This includes mental and emotional stress. Research on cognitive dietary restraint (i.e. worrying and stressing out about food) shows that constantly and negatively fixating on what you eat (or don’t) can have the same unhealthy effect as actually dieting stringently.
Yet we need some stress to actually help with progress and growth, so find your stress sweet spot.
10. Have some self-compassion.
There are going to be meals or days where you don’t eat as you “should”. It’s OK. It happens to everyone. Recognize it, accept it, forgive yourself, and then get back on track.
Research actually shows that self-compassion and flexible eating is associated with lower BMI and a healthier body weight, lower self-reported calorie intake, less anxiety and stress, and a better relationship with food.
Passionate about nutrition and health?
If so, and you’d like to learn more about it, consider the Precision Nutrition Level 1 Certification. Our next group kicks off shortly.
What’s it all about?
The Precision Nutrition Level 1 Certification is the world’s most respected nutrition education program. It gives you the knowledge, systems, and tools to really understand how food influences a person’s health and fitness. Plus the ability to turn that knowledge into a thriving coaching practice.
Developed over 15 years, and proven with over 100,000 clients, the Level 1 curriculum stands alone as the authority on the science of nutrition and the art of coaching.
Whether you’re already mid-career, or just starting out, the Level 1 Certification is your springboard to a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results.
[Of course, if you’re already a student or graduate of the Level 1 Certification, check out our Level 2 Certification Master Class. It’s an exclusive, year-long mentorship designed for elite professionals looking to master the art of coaching and be part of the top 1% of health and fitness coaches in the world.]
Interested? Add your name to the presale list. You’ll save up to 30% and secure your spot 24 hours before everyone else.
We’ll be opening up spots in our next Precision Nutrition Level 1 Certification on Wednesday, April 8th, 2020.
If you want to find out more, we’ve set up the following presale list, which gives you two advantages.
- Pay less than everyone else. We like to reward people who are eager to boost their credentials and are ready to commit to getting the education they need. So we’re offering a discount of up to 30% off the general price when you sign up for the presale list.
- Sign up 24 hours before the general public and increase your chances of getting a spot. We only open the certification program twice per year. Due to high demand, spots in the program are limited and have historically sold out in a matter of hours. But when you sign up for the presale list, we’ll give you the opportunity to register a full 24 hours before anyone else.
If you’re ready for a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results… this is your chance to see what the world’s top professional nutrition coaching system can do for you.
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
Chin-Chance C, et al.Twenty-four-hour leptin levels respond to cumulative short-term energy imbalance and predict subsequent intake. J Clin Endocrinol Metab. 2000 Aug;85(8):2685-91.
Considine RV, et al. Serum immunoreactive-leptin concentrations in normal-weight and obese humans. N Engl J Med. 1996 Feb 1;334(5):292-5.
Doucet E, et al. Evidence for the existence of adaptive thermogenesis during weight loss. Br J Nutr. 2001 Jun;85(6):715-23.
Fogteloo AJ, et al. Effects of recombinant human leptin treatment as an adjunct of moderate energy restriction on body weight, resting energy expenditure and energy intake in obese humans. Diabetes Nutr Metab. 2003 Apr;16(2):109-14.
Hall KD. Modeling Metabolic Adaptations and Energy Regulation in Humans*. Annual review of nutrition. 2012 Aug 21;32:35-54.
Hall KD, et al. Quantification of the effect of energy imbalance on bodyweight. Lancet. 2011 Aug 27;378(9793):826-37.
Hall KD, Jordan PN. Modeling weight-loss maintenance to help prevent body weight regain. The American journal of clinical nutrition. 2008 Dec 1;88(6):1495-503.
Harvie M, et al. The effect of intermittent energy and carbohydrate restriction v. daily energy restriction on weight loss and metabolic disease risk markers in overweight women. Br J Nutr. 2013 Oct;110(8):1534-47.
Heilbronn LK, et al. Effect of 6-mo. calorie restriction on biomarkers of longevity, metabolic adaptation and oxidative stress in overweight subjects. JAMA. 2006 Apr 5; 295(13): 1539–1548.
Helms ER, et al. Evidence-based recommendations for natural bodybuilding contest preparation: nutrition and supplementation. J Int Soc Sports Nutr. 2014 May 12;11:20.
Heymsfield SB, et al. Recombinant leptin for weight loss in obese and lean adults: a randomized, controlled, dose-escalation trial. JAMA. 1999 Oct 27;282(16):1568-75.
Heymsfield SB, Gonzalez MC, Shen W, Redman L, Thomas D. Weight loss composition is one‐fourth fat‐free mass: a critical review and critique of this widely cited rule. Obesity Reviews. 2014 Apr 1;15(4):310-21.
Heymsfield SB, Thomas D, Martin CK, Redman LM, Strauss B, Bosy-Westphal A, Müller MJ, Shen W, Nguyen AM. Energy content of weight loss: kinetic features during voluntary caloric restriction. Metabolism. 2012 Jul 31;61(7):937-43.
Jenkins AB, et al. Carbohydrate intake and short-term regulation of leptin in humans. Diabetologia. 1997 Mar;40(3):348-51.
Joosen AM, Westerterp KR. Energy expenditure during overfeeding. Nutr Metab (Lond). 2006 Jul 12;3:25.
Kelesidis T, Mantzoros CS. The emerging role of leptin in humans. Pediatr Endocrinol Rev. 2006 Mar;3(3):239-48.
Keys AB. The biology of human starvation. University of Minnesota, Laboratory of Physiological Hygiene, 1950.
Leibel RL, et al. Changes in energy expenditure resulting from altered body weight. N Engl J Med. 1995 Mar 9;332(10):621-8.
Leibel RL, Hirsch J. Diminished energy requirements in reduced-obese patients. Metabolism. 1984 Feb;33(2):164-70.
Levine JA, et al. Energy expenditure of nonexercise activity. Am J Clin Nutr. December 2000 72(6): 1451-1454
Levine JA. Non-exercise activity thermogenesis (NEAT). Best Pract Res Clin Endocrinol Metab. 2002 Dec;16(4):679-702.
Levine JA, et al. Non-exercise activity thermogenesis: the crouching tiger hidden dragon of societal weight gain. Arterioscler Thromb Vasc Biol. 2006 Apr;26(4):729-36.
Levine JA, et al. Role of nonexercise activity thermogenesis in resistance to fat gain in humans. Science. 1999 Jan 8;283(5399):212-4.
Livesey G. A perspective on food energy standards for nutrition labelling. Br J Nutr 2001a;85:271–87.
Maclean PS, et al. Biology’s response to dieting: the impetus for weight regain. Am J Physiol Regul Integr Comp Physiol. 2011 Sep;301(3):R581-600.
Mäestu J, et al. Anabolic and catabolic hormones and energy balance of the male bodybuilders during the preparation for the competition. J Strength Cond Res. 2010 Apr;24(4):1074-81.
Myers MG, et al. Mechanisms of leptin action and leptin resistance. Annu Rev Physiol. 2008;70:537-56.
Murgatroyd PR, et al. Leptin does not respond to 48 h fat deposition or mobilization in women. Int J Obes Relat Metab Disord. 2003 Apr;27(4):457-62.
Ravussin E, et al. Determinants of 24-hour energy expenditure in man. Methods and results using a respiratory chamber. J Clin Invest. 1986 Dec;78(6):1568-78.
Rosenbaum M, and Leibel R. Adaptive thermogenesis in humans. Int J Obes (Lond). 2010 Oct; 34(1): S47–S55.
Rosenbaum M, et al. Effects of experimental weight perturbation on skeletal muscle work efficiency in human subjects. Am J Physiol Regul Integr Comp Physiol. 2003 Jul;285(1):R183-92.
Rosenbaum M, et al. Long-term persistence of adaptive thermogenesis in subjects who have maintained a reduced body weight. Am J Clin Nutr. 2008 Oct;88(4):906-12.
Rosenbaum M, et al. Low-dose leptin reverses skeletal muscle, autonomic, and neuroendocrine adaptations to maintenance of reduced weight. J Clin Invest. 2005 Dec;115(12):3579-86.
Rossow LM, et al. Natural bodybuilding competition preparation and recovery: a 12-month case study. Int J Sports Physiol Perform. 2013 Sep;8(5):582-92.
Schoeller DA. The energy balance equation: looking back and looking forward are two very different views. Nutr Rev. 2009 May;67(5):249-54.
Seimon, Radhika V., et al. Intermittent Moderate Energy Restriction Improves Weight Loss Efficiency in Diet-Induced Obese Mice. PLoS One January 19, 2016 DOI: 10.1371/journal.pone.0145157 http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0145157
Smith CF, et al. Flexible vs. Rigid dieting strategies: relationship with adverse behavioral outcomes. Appetite. 1999 Jun;32(3):295-305.
Speakman JR, Westerterp KR. A mathematical model of weight loss under total starvation: evidence against the thrifty-gene hypothesis. Disease Models and Mechanisms. 2013 Jan 1;6(1):236-51.
Stewart TM, et al. Rigid vs. flexible dieting: association with eating disorder symptoms in nonobese women. Appetite. 2002 Feb;38(1):39-44.
Thomas DM, Martin CK, Redman LM, Heymsfield SB, Lettieri S, Levine JA, Bouchard C, Schoeller DA. Effect of dietary adherence on the body weight plateau: a mathematical model incorporating intermittent compliance with energy intake prescription. The American journal of clinical nutrition. 2014 Sep 1;100(3):787-95.
Traoret, CJ, et al. Peanut digestion and energy balance. International Journal of Obesity. 2008;32(2):322-328.
Trexler ET, et al. Metabolic adaptation to weight loss: implications for the athlete. J Int Soc Sports Nutr. 2014 Feb 27;11(1):7.
Varady KA. Intermittent versus daily calorie restriction: which diet regimen is more effective for weight loss? Obes Rev. 2011 Jul;12(7):e593-601.
Westenhoefer J, et al. Cognitive and weight-related correlates of flexible and rigid restrained eating behaviour. Eat Behav. 2013 Jan;14(1):69-72.
Westenhoefer J, et al. Validation of the flexible and rigid control dimensions of dietary restraint. Int J Eat Disord. 1999 Jul;26(1):53-64.
Weyer C, et al. Changes in energy metabolism in response to 48 h of overfeeding and fasting in Caucasians and Pima Indians. Int J Obes Relat Metab Disord. 2001 May;25(5):593-600.
Weyer C, et al. Determinants of energy expenditure and fuel utilization in man: effects of body composition, age, sex, ethnicity and glucose tolerance in 916 subjects. Int J Obes Relat Metab Disord. 1999 Jul;23(7):715-22.
Weyer C, et al. Energy metabolism after 2 y of energy restriction: the biosphere 2 experiment. Am J Clin Nutr. 2000 Oct;72(4):946-53.
The post Can eating too little actually damage your metabolism? Exploring the truths and fallacies of ‘metabolic damage’. appeared first on Precision Nutrition.
Source: Health1
Precision Nutrition co-founder Dr. John Berardi gives you a sneak peek at the Level 2 Certification. Plus, industry leaders share their thoughts on the program.
The post Precision Nutrition Level 2 Certification: A sneak peek into the Precision Nutrition Level 2 Master Class. appeared first on Precision Nutrition.
Source: Health1
Precision Nutrition co-founder Dr. John Berardi gives you a sneak peek at the Level 1 Certification. Plus, industry leaders share their thoughts on the program.
The post Precision Nutrition Level 1 Certification: A sneak peek into the industry’s most respected nutrition certification. appeared first on Precision Nutrition.
Source: Health1
Plenty of people hate kale.
It doesn’t matter that it’s a so-called “superfood.” (And yes, it is pretty super.)
After all, you can’t help what you like… or don’t like.
But should you (or your clients) force down a “superfood” even if you detest it?
Not necessarily.
While it’s popular to put some foods on a pedestal above others, there’s more to healthy eating than just the nutrition facts.
Context matters. Preferences matter. Goals matter.
It’s never as simple as “good” vs. “bad” or “healthy” vs. “unhealthy.”
To show you why, we’ve taken a closer look at five celebrated “superfoods” and their less publicized—and sometimes demonized—counterparts:
- Nutrient-packed kale vs. basically-just-water iceberg lettuce
- Power grain quinoa vs. plain old white rice
- Cancer-fighting blueberries vs. starchy bananas
- Trendy coconut oil vs. kitchen-staple olive oil
- Fat-fighting egg whites vs. cholesterol-boosting whole eggs… or perfectly-balanced whole eggs vs. woefully-incomplete egg whites (depending on your point of view)
You may be surprised at what we found.
Our goal: To empower people to choose what they eat depending on what’s most important to them, not an arbitrary list of food “rules.”
This infographic will help you do just that.

Download this infographic for your tablet or printer to help you (or your clients) stop seeing foods as “good” vs. “bad.”
If you’re a coach, or you want to be…
Learning how to coach clients, patients, friends, or family members through healthy eating and lifestyle changes—in a way that helps them make better food choices while taking their preferences, goals, and lifestyle into account—is both an art and a science.
If you’d like to learn more about both, consider the Precision Nutrition Level 1 Certification. The next group kicks off shortly.
What’s it all about?
The Precision Nutrition Level 1 Certification is the world’s most respected nutrition education program. It gives you the knowledge, systems, and tools you need to really understand how food influences a person’s health and fitness. Plus the ability to turn that knowledge into a thriving coaching practice.
Developed over 15 years, and proven with over 100,000 clients and patients, the Level 1 curriculum stands alone as the authority on the science of nutrition and the art of coaching.
Whether you’re already mid-career, or just starting out, the Level 1 Certification is your springboard to a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results.
[Of course, if you’re already a student or graduate of the Level 1 Certification, check out our Level 2 Certification Master Class. It’s an exclusive, year-long mentorship designed for elite professionals looking to master the art of coaching and be part of the top 1% of health and fitness coaches in the world.]
Interested? Add your name to the presale list. You’ll save up to 30% and secure your spot 24 hours before everyone else.
We’ll be opening up spots in our next Precision Nutrition Level 1 Certification on Wednesday, April 8th, 2020.
If you want to find out more, we’ve set up the following presale list, which gives you two advantages.
- Pay less than everyone else. We like to reward people who are eager to boost their credentials and are ready to commit to getting the education they need. So we’re offering a discount of up to 30% off the general price when you sign up for the presale list.
- Sign up 24 hours before the general public and increase your chances of getting a spot. We only open the certification program twice per year. Due to high demand, spots in the program are limited and have historically sold out in a matter of hours. But when you sign up for the presale list, we’ll give you the opportunity to register a full 24 hours before anyone else.
If you’re ready for a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results… this is your chance to see what the world’s top professional nutrition coaching system can do for you.
The post ‘Superfoods’ vs ‘regular’ foods: Why nutrition facts don’t tell the whole story. [Infographic] appeared first on Precision Nutrition.
Source: Health1
At Precision Nutrition, we don’t tell our clients exactly what to eat—or what not to eat.
In fact, we boldly say: “There are no bad foods.”
Our stance tends to spark lots and lots of questions, which is why we decided to take a deep dive into the whole “good foods vs. bad foods” debate.
In this article we’ll:
- explore how good vs. bad thinking can actually set people up to eat MORE of the “bad” foods
- offer an alternative way to think about sweets, chips, and other low-nutrient foods
- provide techniques we use to help to liberate clients from the good vs. bad mindset.
We’ll be honest. The “no bad foods” philosophy can be really scary, especially for people who’ve spent years organizing foods into good and bad categories.
But it can also be equally transformative.
We’ve found that once our clients welcome the foods they love back into their lives—without fear and without guilt—they struggle less, enjoy eating more, and, finally, are able to overcome obstacles that stand between them and their healthy eating goals.
Why the good vs. bad approach just doesn’t work.
Many people divide food into just two categories.
Good foods: Vegetables, legumes, whole grains, fish, lean meat, and other minimally-processed, nutrient-dense foods.
Bad foods: Sweets, chips, crackers, white bread, fries, and other highly-processed foods that offer little to no nutritional value.
And before we explain why we don’t sort food into “good” and “bad” buckets, we want to be very clear. The nutritional differences between these two categories are quite easy to spot.
Many of the so-called “bad” foods, in high amounts, can raise the risk for a variety of diseases.
They’re also incredibly hard to resist. (The food industry really has created cheap, easily accessible products that our taste buds and brains love.)
But are they bad?
We don’t use that terminology—for six major reasons.
Reason #1: One single food doesn’t define your entire diet.
Maybe you’ve heard of a teenager who ate just four foods for most of his life: fries, chips, white bread, and processed pork.1
And then he went blind.
It’s a cautionary tale, for sure, but it’s important to keep one thing in perspective: That teen is an outlier. Most people don’t eat just four foods.
They eat a variety.
And the fries, chips, bread, and pork didn’t cause the teen’s blindness directly.
They caused it indirectly—by crowding out foods needed for good eye health.
What truly matters for good health? Balance.
In other words, you don’t want your toaster pastries, spray cheese-like product, and crescent rolls to crowd out veggies, fruit, beans, nuts, fresh meats, seafood, and other nutrient-dense whole foods.
If they do, like the teen we mentioned, you run the risk of deficiency.
So the question is: Are you in balance?
We experience massive benefits (fat loss, improved health) when we go from poor nutrition to average or above average.
But eventually, we see diminishing returns.
As this chart shows, not only are gains much harder to see after 80 to 90 percent of your diet is composed of whole, minimally-processed foods, you also run the risk of eating disorders like orthorexia (an unhealthy obsession with healthy eating).

Is most (80 to 90 percent) of what you eat nutrient-dense and minimally processed? (Think veggies, fruit, meat, fish, nuts, seeds, beans, lentils, whole grains.) Then there’s likely room for less nutritious foods.
Is most of what you eat highly-processed and nutrient-poor? (Think sweets and chips.) Consider small actions to make your diet just a little bit better. Slowly add more nutrient-dense foods (veggies, fruit, fish, poultry, and so on) to each meal. Use our “What Should I Eat?” infographic for guidance.
Reason #2: No one food is bad for all people in all situations.
To illustrate this point, Precision Nutrition Master Coach Kate Solovieva often brings up cola.
Many people see it as a bad food. Because it’s loaded with sugar and lacking in vitamins and minerals.
But is cola bad in all situations?
“Let’s say you’re visiting a country with no safe drinking water,” says Solovieva. “In that case, cola—with its air-tight seal—is a much better option than water.”
Or, maybe you’re sixty sweaty miles into a 100-mile bike race and your blood sugar is so low that you’re hallucinating flying pink elephants. In that case, the sugar and caffeine in the cola might make the difference between finishing the race and a DNF.
Our individual physiology and psychology also affect what happens when we eat specific foods.
Added sugar, for example, affects someone with type 2 diabetes differently than it affects someone whose cells are insulin sensitive. And it can affect the same person differently depending on whether they’re sleep deprived.
At PN, we talk a lot about deep health—which describes so much more than our weight, cholesterol level, and blood sugar.
Deep health includes where we live and how we feel and who we spend time with. It’s about every aspect of who we are.
When you consider health in this light, the exact foods become less important, and the overall eating pattern and full context of someone’s life becomes a lot more important.
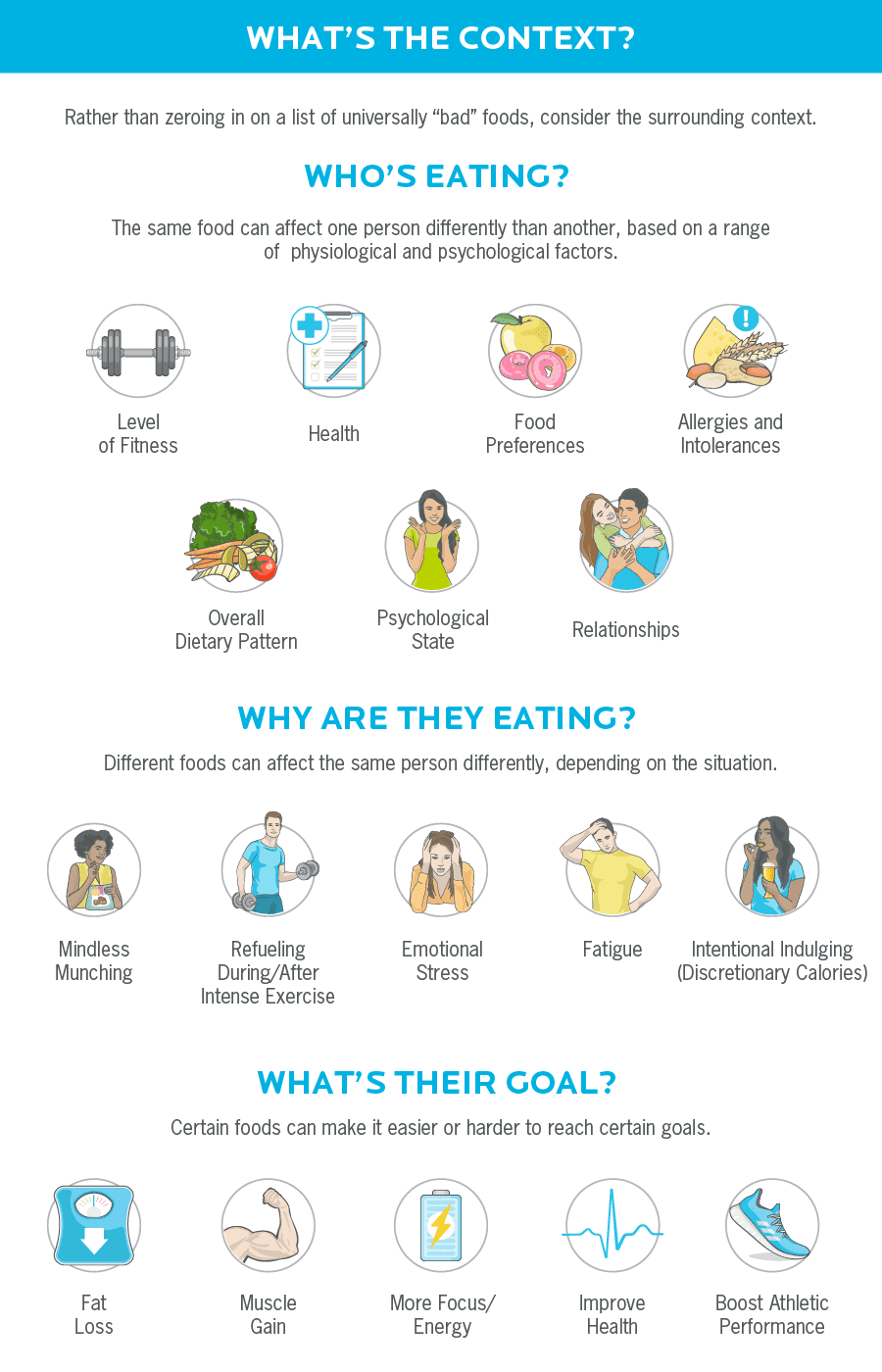
Reason #3: Demonizing certain foods can make them even more appealing.
Lots of people tell us that 100 percent abstaining from “bad foods” is the only way they can maintain any smidgen of control around their eating.
If they say “okay” to one “bad” food, they worry they’ll open the floodgates to a diet swollen with cookies, brownies, chips, and fries—as well as devoid of veggies and other whole foods.
Here’s the thing:
There’s a subtle difference between demonizing a food and merely abstaining from it because you know you tend to overeat it.
When we demonize foods, we “moralize these foods—thinking of ourselves as bad people for eating them,” says Solovieva.
This paradoxically can increase our desire for the very foods we’re trying not to eat. When researchers from Arizona State University showed dieters negative messages about unhealthy foods, the dieters experienced increased cravings for those foods—and ate more of them.2
It’s true that some people can restrict certain “bad” foods for a while.
But, for a lot of people, cravings eventually overwhelm their ability to restrict. And when they eat something “bad”—they feel guilty. So they eat even more—and may even stop trying to reach their goals. This can create a vicious circle, as the graphic below shows.
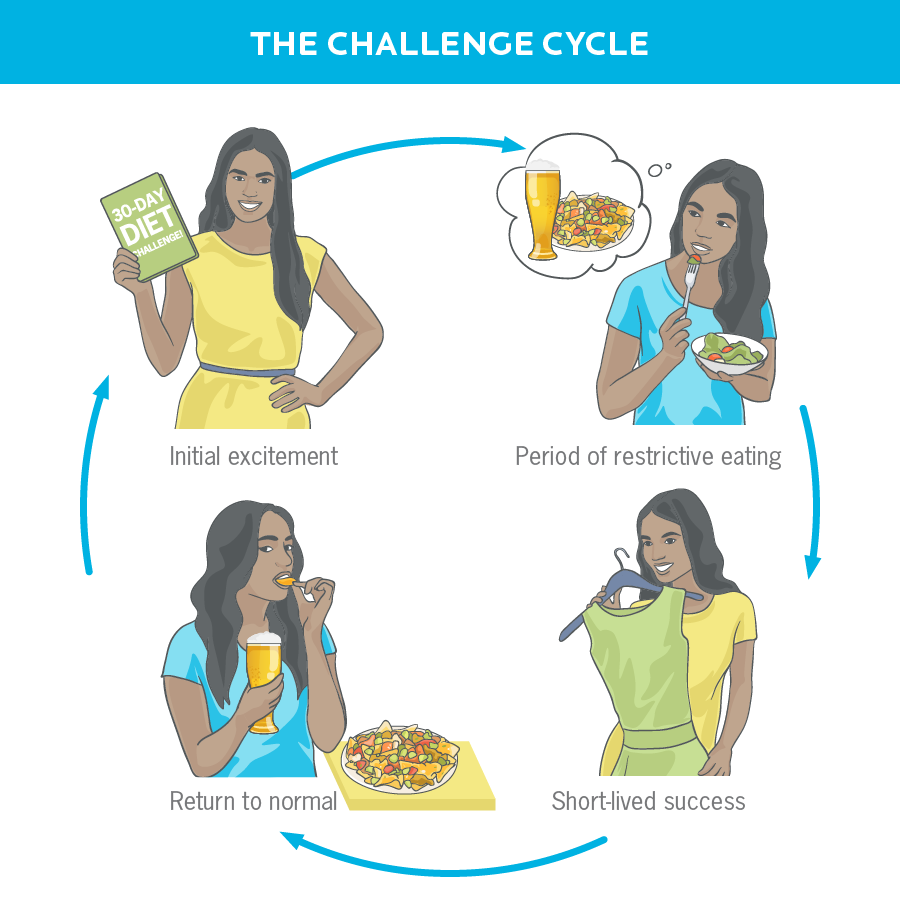
Now, let us be clear: For some people, certain foods may not be worth the struggle—at least for now. They may decide that, if they’re around certain foods, they’re going to overeat them. So they get them out of the house.
And that strategy can work. In fact, we encourage our clients to do kitchen makeovers and remove foods they tend to overeat.
But it’s not the same thing as labeling a food as “bad.”
When we label foods “something I tend to overeat” rather than “bad,” we’re better able to relax, remain flexible, and, potentially, grow into someone who can enjoy the same food, in moderation.
Reason #4: Categorizing foods as “good” and “bad” can work—but usually only for a while.
Having coached more than 100,000 clients, we can say with confidence that “all or nothing” rarely gets us “all.”
Instead, it often gets us nothing.
For example, when someone decides to stop eating “bad” foods, usually they try really hard to stay true to their goal. They’re committed, and they even may stick to avoiding a long list of forbidden foods… for a bit.
But then something goes wrong.
Maybe they go to work and find that a coworker left homemade brownies on their desk.
Or every part of their day goes sideways and, in the evening, they find themselves head down in a gallon of chocolate chip cookie dough as they think “This is bad.”
Or they’re driving for hours to visit relatives, pull into a rest stop, and all they find to eat: the stuff on their forbidden foods list.
Rigidity—good or bad, all or nothing—is the enemy of consistency.
But on the flipside, flexibility helps you stay more consistent. That’s because it allows you to lean into all the solutions available to you.
Flexibility also frees people to use internal guidance—rather than someone else’s external rules—to decide what foods to eat, when to eat them, and why.
So, for example, rather than avoiding sugar just because a health site told them to stop eating it, someone might consider:
- Am I hungry?
- Am I stressed?
- Is this food worth it to me?
- What else have I eaten today?
- What would allow me to truly enjoy this food—without going overboard?
That internal guidance might allow that person with the brownie to say, “You know, I really like brownies, but I’m going to save this until after lunch, when I’m not as hungry, so I can eat it slowly and truly savor it.”
Or that person who is head down in the gallon of ice cream to say, “Okay, so this was probably more ice cream than my body really needed. True. No getting around that. How can I avoid feeling this triggered in the future? And are there other ways I can comfort myself that don’t involve raiding the freezer?”
And for that person at the rest stop, flexibility allows them to scan their choices and opt for the best meal for them at that moment.
Reason #5: It’s really okay—and completely normal—to eat for pleasure.
Food serves many purposes far beyond just flooding someone’s body with nutrients and calories.
Some foods aren’t necessarily loaded with nutrients, but they:
- Taste amazing.
- Connect us with friends and families.
- Create a sense of belonging.
- Make celebrations worthwhile.
In other words, food isn’t just fuel. It’s also love and culture and pleasure—and a whole lot more.
When you think about food in this way, everything—even your grandma’s special black forest cake—can have a purpose and a place.
Rather than a list of foods you can or can’t eat, you instead have choices. You have foods you choose to eat for energy, for pleasure, for health, and many other important reasons.
Reason #6: When we obsess over “bad foods,” we rob ourselves of the ability to evolve.
Rigidly abstaining can teach us to get really good at… abstaining.
And if you’re okay with abstaining from a long list of foods for the rest of your life, there’s nothing wrong with that approach.
But if you’re not okay with a life sentence of no cookies, no brownies, no cake, no bread, and no pasta, then you may be happy to learn that there’s an alternative approach. It involves getting curious about why you struggle to moderate your consumption of certain foods.
Consider:
What leads to feeling out-of-control?
What triggers the “I need this” and the “I can’t stop eating this” thoughts?
When is it possible to eat this food in moderate amounts (if ever)? When isn’t it?
The point: Rather than zeroing in on “bad foods,” look for the underlying reasons (called triggers) that lead you to struggle.
A trigger can be a:
- Feeling. We might eat more when we’re stressed, lonely, or bored. Food fills the void.
- Time of day. We always have a cookie at 11 am, or a soda at 3 pm. It’s just part of our routine.
- Social setting. Hey, everyone else is having beer and chicken wings, so might as well join the happy hour!
- Place. For some reason, a dark movie theater or our parents’ kitchen might make us want to munch.
- Thought pattern. Thinking “I deserve this” or “Life is too hard to chew kale” might steer us toward the drive-thru window.
To uncover triggers, we often ask our clients to keep a food journal—writing down everything they eat and drink for a week or two. When they find themselves craving or feeling out of control, we ask them to jot down the answers to questions like:
- What am I feeling?
- What time is it?
- Who am I with?
- Where am I?
- What thoughts am I having?
They approach it with a “feedback not failure” mentality.
The point isn’t to catch them doing something wrong. It’s to help them assess what’s really going on.
Once we understand why our clients are reaching for these foods, we’re better-equipped to suggest actions that truly help them move towards a healthier relationship with all foods.
One Man’s Evolution Away From Bad Foods
Dominic Matteo grew up reading bodybuilding magazines. For most of his life, he thought of veggies, chicken breast, egg whites, sweet potatoes, oats, and a few other foods as “good.”
All other foods? Bad.
These distinctions didn’t bother him when he wasn’t trying to shed fat.
But once he started trying to restrict his intake, the label “bad” functioned like a tractor beam that drew him straight to the ice cream.
“That’s when I was like, ‘Oh, this is a problem,’” he says.
For several months, he completely abstained from all sweets. He just didn’t eat sugar—at all.
But he knew that wasn’t a sustainable—or enjoyable—way to live.
After applying Precision Nutrition strategies, however, Matteo started to view his list of bad foods differently. Rather than seeing ice cream as “bad,” he thought of it as “a food I enjoy, but slows my progress.”
That new label allowed him to consider how and under what conditions he would coexist with this sweet treat.
“Now, if I do eat it, it will be under certain conditions that I can feel happy about,” he says.
For example, he loves to indulge in ice cream from shops that make it fresh that day. But lower-quality ice cream isn’t worth it for him.
Today, Matteo is more than 100 pounds lighter and, as a Precision Nutrition Master Coach, he’s helping others to follow in his footsteps.
“If there are no good or bad foods, how can anyone ever know what to eat—and what to limit?”
We hear this a lot.
That’s because some people assume that “no bad foods” is synonymous with “all foods are good so eat whatever you want.”
But that’s not what we’re saying at all.
We are, however, saying this: Rather than sorting food into just two buckets—good and bad—it’s usually more helpful for most people to see food as a continuum of eat more, eat some, and eat less.
This might, at first, merely sound like another way to sort food into categories.
But it’s not.
Unlike lists of bad foods, which tend to be universally rigid, a continuum “allows everything to be contextual and personalized,” explains Precision Nutrition Master Coach Dominic Matteo.
“If my goal is muscle gain, my continuum will look different than if my goal is fat loss,” Matteo says.
Once people define that continuum for themselves, we then work with them to find ways to include more “eat more” foods and fewer “eat less” foods, aiming to make each meal just a little bit better.
For example, before Matteo became a Precision Nutrition Master Coach, he was a client who wanted to lose fat. This is how “just a little bit better” looked like for him for a specific fast food lunch.

He eventually ended up in a similar place that some forbidden foods lists may have sent him, but he did it in small steps, and in a way that was ultimately more sustainable.
What’s more, it didn’t mean he could never have a double bacon cheeseburger again. Sometimes he does, but he enjoys it—on his terms.
“My client believes in bad foods—as if they were a religion. Help!”
Saying, “there are no bad foods” usually results in a blank stare.
So, pretend you don’t know the answers, says Kate Solovieva.
Assume a poker face, and ask questions that seem obvious.
What follows is a conversation Solovieva had with a client about this very topic.
Client: Bad foods are my problem. I need to cut them out. I just can’t eat them.
Coach: So, can you tell me a little bit more. When you talk about cutting out the bad foods, what does that look like?
Client: Taking sugar out of my diet.
Coach: So when you say sugar, what are some of the things you are thinking of?
Client: Cookies. Pastries. Chocolate—chocolate is my weakness.
Coach: So… you really enjoy chocolate?
Client: I do.
Coach: Help me understand. What is it that you enjoy?
Client: I don’t know if it’s the rush of eating the chocolate bar itself. Or maybe it’s the fact that I don’t have it all the time. I don’t know. There’s something about chocolate.
Coach: So, in some ways, it makes you feel super good. And it obviously gives you pleasure. What makes you label it as bad?
Client: It’s the high-calorie count and the amount—the portion.
Coach: So the high number of calories makes it bad? Can you explain?
Client: Well, for me, it leads to weight gain.
Coach: So what I am hearing is that it’s not the chocolate that’s bad. It’s the weight gain that’s bad. Is that right?
Client: Pretty much. Exactly.
Coach: So I’m curious about something you said. You love chocolate. You enjoy it. You like the taste of it. When I asked why it’s bad, you told me about the calories and the portions. Can you tell me more?
Client: Well, I can’t just have one or two squares. Ideally I should have no more than five squares—half a bar. But I don’t have that control. The moment I taste it, I have to have more and more and more.
Coach: So what happens when you don’t have chocolate at all?
Client: I’ve gone months without it. And it’s great! But then I end up eating it—like on a special occasion. And then I binge. And then everything goes downhill. So I’m better off not having it at all.
Coach: What do you think would happen if you had a little bit… everyday? Like on purpose.
Client: I don’t know…I don’t think I have that control. Should I try that?
Coach: I don’t know. Should you?
Client: (Sounding tentative) Sure, maybe I can try that?
Coach: Well, what I am hearing is that you enjoy it. And it sounds like the bingeing behavior is happening because you don’t have it every day. So maybe you can try this as an experiment. Maybe you see what happens if, every single day, you have this thing that you enjoy. And when you eat it, if you want more, you can just remind yourself that you can have more—tomorrow. Are you with me?
Client: Yes.
Coach: It’s a scary experiment. But if you decide to give it a shot, let me know, okay?
Client: Okay, I will. I’m kinda nervous about it, but I will try it.
And then the conversation can go on to define the experiment: How much chocolate? What time of day? How will you eat it?
And no matter what the client ultimately does—whether the client tries the suggestion or not—“you’re in a position for them to come back to you without feeling judged,” Solovieva says.
“Isn’t it just easier to not eat certain foods?”
For some people in some situations at certain points in their journey: yes.
But this need to abstain doesn’t have to be a permanent situation. Once they develop a range of habits, many people can shift from abstaining from certain foods to moderating them.
That’s why we like to ask our clients to consider two questions about the foods they think of as bad:
What does this food do—for you?
What would you like it to do?
For example, maybe, right now, certain foods make you feel out of control because you struggle to stop eating them once you start. But you’d like them to merely become foods you enjoy in moderation.
What are all of the possible ways of going from point A (out of control) to point B (something I enjoy in moderation)?
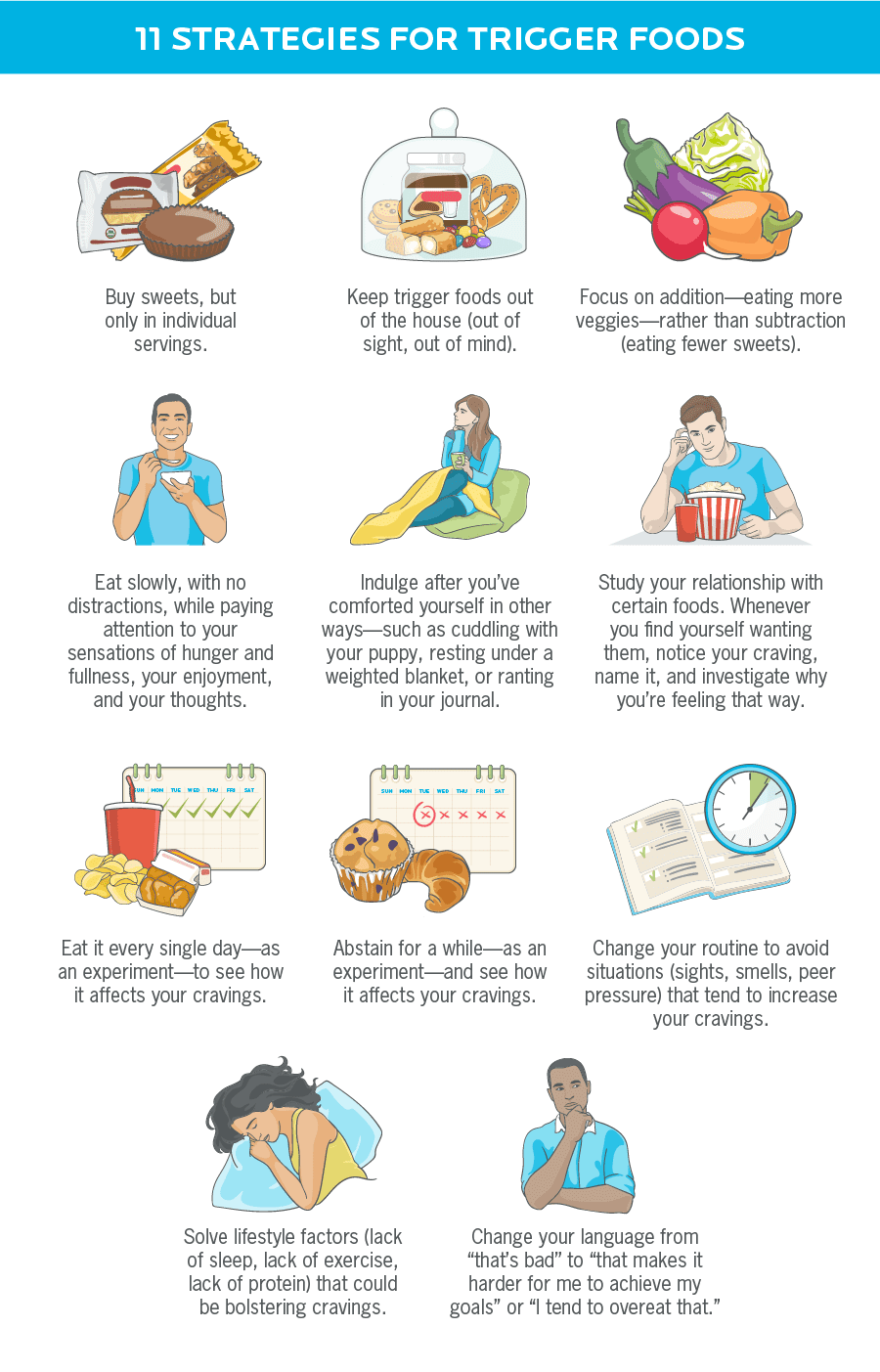
There are dozens of other possibilities that we didn’t even list on the chart above. You might try one. You might try several. You might try all of them.
The point: You may find that liberating yourself from the good vs. bad mindset frees you to see more possibilities than ever before.
And, along the way, you may also discover that this broader, more flexible mindset allows you not only to enjoy every meal a heck of a lot more—but also to reach your goals more quickly.
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
- Harrison R, Warburton V, Lux A, Atan D. Blindness Caused by a Junk Food Diet. Ann Intern Med [Internet]. 2019 Sep 3; Available from: http://dx.doi.org/10.7326/L19-0361
- Pham N, Mandel N, Morales AC. Messages from the Food Police: How Food-Related Warnings Backfire among Dieters. Journal of the Association for Consumer Research. 2016 Jan 1;1(1):175–90.
If you’re a coach, or you want to be…
Learning how to coach clients, patients, friends, or family members through healthy eating and lifestyle changes—in a way that gives them flexiblity based on their personal preferences—is both an art and a science.
If you’d like to learn more about both, consider the Precision Nutrition Level 1 Certification. The next group kicks off shortly.
What’s it all about?
The Precision Nutrition Level 1 Certification is the world’s most respected nutrition education program. It gives you the knowledge, systems, and tools you need to really understand how food influences a person’s health and fitness. Plus the ability to turn that knowledge into a thriving coaching practice.
Developed over 15 years, and proven with over 100,000 clients and patients, the Level 1 curriculum stands alone as the authority on the science of nutrition and the art of coaching.
Whether you’re already mid-career, or just starting out, the Level 1 Certification is your springboard to a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results.
[Of course, if you’re already a student or graduate of the Level 1 Certification, check out our Level 2 Certification Master Class. It’s an exclusive, year-long mentorship designed for elite professionals looking to master the art of coaching and be part of the top 1% of health and fitness coaches in the world.]
Interested? Add your name to the presale list. You’ll save up to 30% and secure your spot 24 hours before everyone else.
We’ll be opening up spots in our next Precision Nutrition Level 1 Certification on Wednesday, April 8th, 2020.
If you want to find out more, we’ve set up the following presale list, which gives you two advantages.
- Pay less than everyone else. We like to reward people who are eager to boost their credentials and are ready to commit to getting the education they need. So we’re offering a discount of up to 30% off the general price when you sign up for the presale list.
- Sign up 24 hours before the general public and increase your chances of getting a spot. We only open the certification program twice per year. Due to high demand, spots in the program are limited and have historically sold out in a matter of hours. But when you sign up for the presale list, we’ll give you the opportunity to register a full 24 hours before anyone else.
If you’re ready for a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results… this is your chance to see what the world’s top professional nutrition coaching system can do for you.
The post We’ve told 100,000 clients, “There are no bad foods.” And we’re not about to stop. Here’s why. appeared first on Precision Nutrition.
Source: Health1
Some vegans believe meat causes cancer and destroys the planet. But meat-eaters often argue that giving up animal foods leads to nutritional deficiencies. Both sides say their approach is healthier. What does science say? And how can you best help clients, no matter their dietary preferences? Keep reading for the answers.
++++
Put a group of vegans and Paleo enthusiasts in the same social media thread, and one thing is nearly 99 percent certain: They’ll start arguing about food.
“Meat causes cancer!”
“You need meat for B12!”
“But meat production leads to climate change!”
“Meat-free processed food is just as bad!”
And on it will go.
Let’s just say that, when it comes to the vegan vs. meat-eater debate, people have thoughts, and they feel strongly about them.
Who’s right?
And which approach is right for you?
And what should you tell your clients?
As it turns out, the answers to those questions are nuanced.
In this article, you’ll find our take on the vegetarian vs. meat-eater debate, which you may find surprising—potentially even shocking—depending on your personal beliefs.
You’ll learn:
- The real reasons plant-based diets may lower risk for disease.
- Whether eating red and processed meat raises risk for certain diseases.
- How to eat for a better planet.
- Why some vegetarians feel better when they start eating meat—and, conversely, why some meat-eaters feel better when they go vegetarian.
- How to help your clients (or yourself) weigh the true pros and cons of each eating approach.
Vegan vs. vegetarian vs. plant-based vs. omnivore: What does it all mean?
Different people use plant-based, vegetarian, vegan, and other terms in different ways. For the purposes of this article, here are the definitions we use at Precision Nutrition.
Plant-based diet: Some define this as “plants only.” But our definition is broader. For us, plant-based diets consist mostly of plants: vegetables, fruits, beans/legumes, whole grains, nuts, and seeds. In other words, if you consume mostly plants with some animal-based protein, Precision Nutrition would still consider you a plant-based eater.
Whole-food plant-based diet: A type of plant-based diet that emphasizes whole, minimally processed foods.
Fully plant-based / plant-only diet: These eating patterns include only foods from the plant/fungi kingdom without any animal products. Fully plant-based eaters don’t consume meat or meat products, dairy, or eggs. Some consume no animal byproducts at all—including honey.
Vegan diet: A type of strict, fully plant-based diet that tends to include broader lifestyle choices such as not wearing fur or leather. Vegans often attempt to avoid actions that bring harm or suffering to animals.
Vegetarian diet: “Vegetarian” is an umbrella term that includes plant-only diets (fully plant-based / plant-only / vegan) as well as several other plant-based eating patterns:
- Lacto-ovo vegetarians consume dairy and eggs.
- Pesco-pollo vegetarians eat fish, shellfish, and chicken.
- Pescatarians eat fish and shellfish.
- Flexitarians eat mostly plant foods as well as occasional, small servings of meat. A self-described flexitarian seeks to decrease meat consumption without eliminating it entirely.
Omnivore: Someone who consumes a mix of animals and plants.
Now that we know what the terms mean, let’s turn to the controversy at hand.
The Health Benefits of Vegetarian vs. Omnivore Diets
Many people assume that one of the big benefits of plant-only diets is this: They reduce risk for disease.
And a number of studies support this.
For example, when researchers in Belgium asked nearly 1500 vegans, vegetarians, semi-vegetarians, pescatarians, and omnivores about their food intake, they found that fully plant-based eaters scored highest on the Healthy Eating Index, which is a measure of dietary quality.
Omnivores (people who eat at least some meat) scored lowest on the Healthy Eating Index and the other groups scored somewhere in between. Meat eaters were also more likely than other groups to be overweight or obese.1
Other research has also linked vegetarian diets with better health indicators, ranging from blood pressure to waist circumference.2
So, is the case closed? Should we all stop eating steaks, drinking lattes, and making omelets?
Not necessarily.
That’s because your overall dietary pattern matters a lot more than any one food does.
Eat a diet rich in the following foods and food groups and it likely doesn’t matter all that much whether you include or exclude animal products:
- minimally-processed whole foods
- fruits and vegetables
- protein-rich foods (from plants or animals)
- whole grains, beans and legumes, and/or starchy tubers (for people who eat starchy carbs)
- nuts, seeds, avocados, extra virgin olive oil, and other healthy fats (for people who eat added fats)
Of the foods we just mentioned, most people—and we’re talking more than 90 percent—do not consume enough of one category in particular: fruits and vegetables. Fewer than 10 percent of people, according to the Centers for Disease Control, eat 1.5 to 2 cups of fruit and 2 to 3 cups of vegetables a day.3
In addition, other research has found that ultra-processed foods (think chips, ice cream, soda pop, etc.) now make up nearly 60% of all calories consumed in the US.4
Fully plant-based eaters score higher on the Healthy Eating Index not because they forgo meat, but rather because they eat more minimally-processed whole plant foods such as vegetables, fruits, beans, nuts, and seeds.
Since it takes work—label reading, food prep, menu scrutiny—to follow this eating style, they may also be more conscious of their food intake, which leads to healthier choices. (Plant-based eaters also tend to sleep more and watch less TV, which can also boost health.)
And meat-eaters score lower not because they eat meat, but because of a low intake of whole foods such as fish and seafood, fruit, beans, nuts, and seeds. They also have a higher intake of refined grains and sodium—two words that usually describe highly-processed foods.
Meat-eaters, other research shows, also tend to drink and smoke more than plant-based eaters.5
In other words, meat may not be the problem. A diet loaded with highly-processed “foods” and virtually devoid of whole, plant foods, on the other hand, is a problem, regardless of whether the person following that diet eats no meat, a little meat, or a lot of meat.6
Now check out the middle of the Venn diagram below. It highlights the foundational elements of a healthful diet that virtually everyone agrees on, no matter what their preferred eating style.
These are the nutritional choices that have the greatest positive impact on your health.
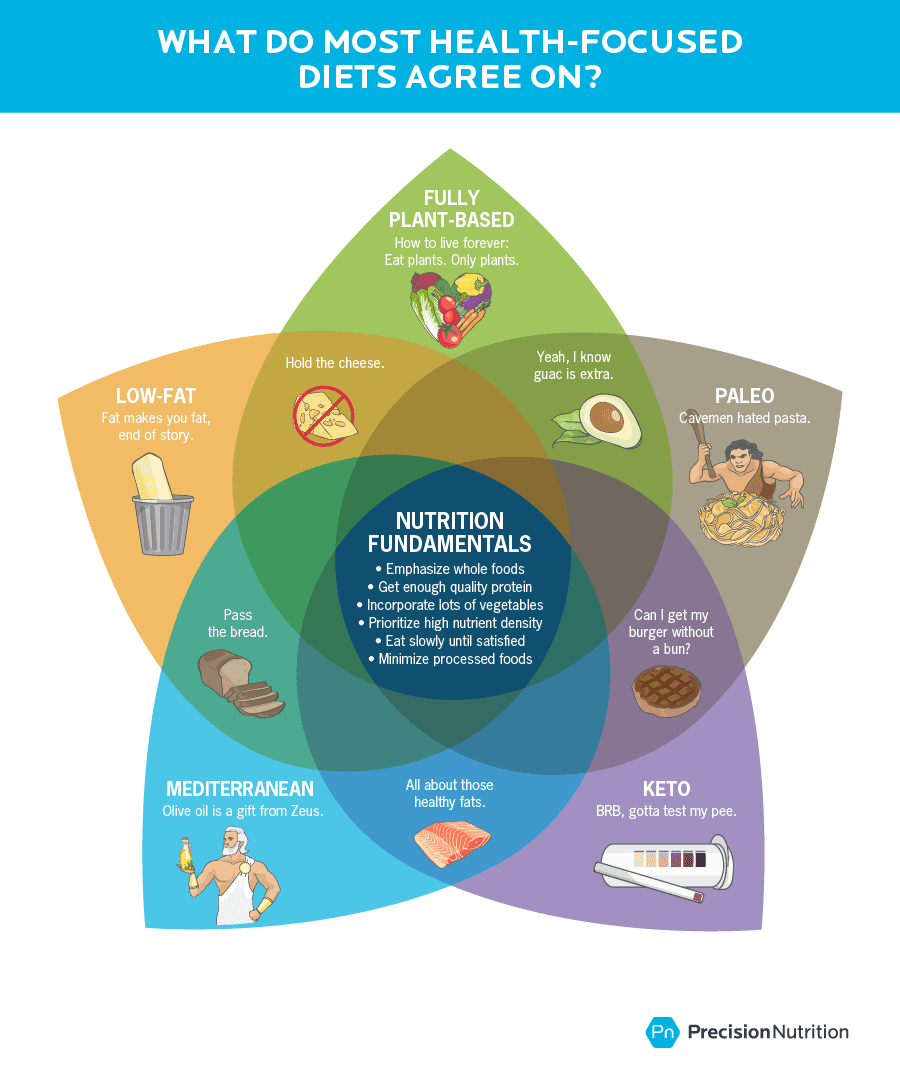
Does meat cause cancer?
For years, we’ve heard that meat-eating raises risk for cancer, especially when it comes to red and processed meat.
And research suggests that red and processed meat can be problematic for some people.
Processed meat—lunch meat, canned meat, and jerky—as well as heavily grilled, charred, or blackened red meat can introduce a host of potentially carcinogenic compounds to our bodies.7,8 (This article offers a deeper dive into these compounds.)
Several years ago, after reviewing more than 800 studies, the International Agency for Research on Cancer (IARC), a part of the World Health Organization, determined that each daily 50-gram portion of processed meat—roughly the amount of one hotdog or six slices of bacon—increased risk of colon cancer by 18 percent.
They listed red meat as “probably carcinogenic” and processed red meat as “carcinogenic,” putting it in the same category as smoking and alcohol.9
So no more bacon, baloney, salami, or hotdogs, right?
Again, maybe not.
First, we want to be clear: We don’t consider processed meat a health food. In our Precision Nutrition food spectrum, we put it in the “eat less” category.
But “eat less” is not the same as “eat never.”
Why? Several reasons.
First, the research is a bit murky.
Several months ago, the Nutritional Recommendations international consortium, made up of 14 researchers in seven countries, published five research reviews based on 61 population studies of more than 4 million participants, along with several randomized trials, to discern the link between red meat consumption and disease.
Cutting back on red meat offered a slim benefit, found the researchers, resulting in 7 fewer deaths per 1000 people for red meat and 8 fewer deaths per 1000 people for processed meat.10
(The study’s main author, though, has been heavily criticized for having ties to the meat industry. Some people have also questioned his methods. This article provides an in-depth analysis.)
Overall, the panel suggested that adults continue their current red meat intake (both processed and unprocessed), since they considered the evidence against both types of meat to be weak, with a low level of certainty.
In their view, for the majority of individuals, the potential health benefits of cutting back on meat probably do not outweigh the tradeoffs, such as:
- impact on quality of life
- the burden of modifying cultural and personal meal preparation and eating habits
- challenging personal values and preferences
Second, the IARC does list processed meat in the same category as cigarettes—because both do contain known carcinogens—but the degree that they increase risk isn’t even close.
To fully explain this point, we want to offer a quick refresher on two statistical terms—“relative risk” and “absolute risk”—that many people tend to confuse.
Relative risk vs. absolute risk: What’s the difference?
In the media, you often hear that eating X or doing Y increases your risk for cancer by 20, 30, even 50 percent or more. Which sounds terrifying, of course.
But the truth? It depends on what kind of risk they’re talking about: relative risk or absolute risk. (Hint: It’s usually relative risk.)
Let’s look at what each term means and how they relate to each other.
Relative risk: The likelihood something (such as cancer) will happen when a new variable (such as red meat) is added to a group, compared to a group of people who don’t add that variable.
On average, studies have found that every 50 grams of processed red meat eaten daily—roughly equivalent to one hot dog or six slices of bacon—raises relative risk for colon cancer by about 18 percent.11
Like we said, that certainly sounds scary.
But keep reading because it’s not as dire as it seems.
Absolute risk: The amount that something (such as red meat) will raise your total risk of developing a problem (such as cancer) over time.
Your absolute risk for developing colon cancer is about 5 percent over your lifetime. If you consume 50 grams of processed red meat daily, your absolute risk goes up to 6 percent. This is a 1 percent rise in absolute risk. (Going from 5 percent to 6 percent is, you guessed it, an 18 percent relative increase.)
So, back to smoking. Smoking doubles your risk of dying in the next 10 years. Smoking, by the way, also accounts for 30 percent of all cancer deaths, killing more Americans than alcohol, car accidents, suicide, AIDS, homicide, and illegal drugs combined.
That’s a lot more extreme than the 1 percent increase in lifetime risk you’d have by eating a daily hot dog.
Finally, how much red and processed meat raises your risk for disease depends on other lifestyle habits—such as exercise, sleep, and stress—as well as other foods you consume.
Getting plenty of sleep, exercising regularly, not smoking, and eating a diet rich in vegetables, fruits and other whole foods can mitigate your risk.
Is processed meat the best option around? No.
Must you completely part ways with bacon, ham, and franks? No.
If you have no ethical issues with eating animals, there’s no need to ban red and processed meat from your dinner plate. Just avoid displacing other healthy foods with meat. And keep intake moderate.
Think of it as a continuum.
Rather than eating less meat, you might start by eating more fruits and vegetables.
You might go on to swap in whole, minimally-processed foods for ultra-processed ones.
Then you might change the way you cook meat, especially the way you grill.
And then, if you want to keep going, you might look at reducing your intake of processed and red meat.
Okay, but at least plants are better for the planet. Right?
The answer, yet again, is pretty nuanced.
Generally speaking, consuming protein from animals is less efficient than getting it straight from plants. On average, only about 10 percent of what farm animals eat comes back in the form of meat, milk, or eggs.
Unlike plants, animals also produce waste and methane gasses that contribute to climate change. “Raising animals for slaughter requires a lot of resources and creates a lot of waste,” explains Ryan Andrews, MS, MA, RD, CSCS, author of A Guide to Plant-Based Eating and adjunct professor at SUNY Purchase.
For those reasons, a gram of protein from beef produces roughly 7.5 times more carbon than does a gram of protein from plants. Cattle contribute to about 70 percent of all agricultural greenhouse gas emissions, while all plants combined contribute to just 4 percent.12
But that doesn’t necessarily mean you must completely give up meat in order to save the planet. (Unless, of course, you want to.)
For a 2019 study in the journal Global Environmental Change, researchers from Johns Hopkins and several other universities looked at the environmental impact of nine eating patterns ranging from fully plant-based to omnivore.13
Notably, they found:
- Reducing meat intake to just one meal a day cuts your environmental impact more than does a lacto-ovo vegetarian diet.
- An eating pattern that includes small, low on the food chain creatures—think fish, mollusks, insects, and worms—poses a similar environmental impact as does a 100 percent plant-only diet.
In other words, if reducing your environmental impact is important to you, you don’t necessarily need to go fully plant-based to do it. You could instead try any of the strategies below.
(And if you’re not interested in taking environmental actions right now, that’s totally okay, too. Ultimately, that’s a personal choice.)
5 ways to reduce the environmental impact of your diet
1. Limit your meat intake.
Consider capping your consumption at 1 to 3 ounces of meat or poultry a day and your consumption of all animal products to no more than 10 percent of total calories, suggests Andrews.
For most people, this one strategy will reduce meat intake by more than half. Replacing meat with legumes, tubers (such as potatoes), roots, whole grains, mushrooms, bivalves (such as oysters), and seeds offers the most environmental benefit for your buck.
2. Choose sustainably raised meat, if possible.
Feedlot animals are often fed corn and soy, which are generally grown as heavily-fertilized monocrops. (Monocropping uses the same crop on the same soil, year after year).
These sorts of heavily fertilized crops lead to nitrous oxide emissions, a greenhouse gas, but crop rotation (changing the crops that are planted from season to season) can reduce these greenhouse gasses by 32 to 315 percent.14
Cattle allowed to graze on grasses (which requires a considerable amount of land), on the other hand, offer a more sustainable option, especially if you can purchase the meat locally.
3. Eat more meals at home.
Homemade meals require less packaging than commercially-prepared ones, and they also tend to result in less food waste.
4. Purchase locally-grown foods.
In addition to reducing transportation miles, local crops tend to also be smaller and more diversified. Veggies grown in soil also produce fewer emissions than veggies grown in greenhouses that use artificial lights and heating sources.
5. Slash your food waste.
As food rots in landfills, it emits greenhouse gasses. “Wasted food is a double environmental whammy,” explains Andrews. “When we waste food, we waste all of the resources that went into producing the food. When we send food to the landfill, it generates a lot of greenhouse gases.”
The Impossible Burger? Or the Imposter Burger?
Made from plant proteins (usually wheat, pea, lentils, or soy) and heme (the iron-containing compound that makes meat red), several meat-like foods have popped up recently, including the Impossible Burger and the Beyond Meat Burger.
So should you give up beef burgers and opt to eat only Impossible Burgers (or another plant-based brand) instead?
The answer depends on how much you like beef burgers.
That’s because the Impossible Burger is not healthier than a beef burger. It’s just another option.
It contains roughly the same number of calories and saturated fat as a beef burger. It also has more sodium and less protein.
And, much like breakfast cereal, it’s fortified with some vitamins, minerals, and fiber.
Rather than a health food, think of the Impossible Burger as a meat substitute that doesn’t come from a farm dependent on prophylactic antibiotics, which can lead to antibiotic resistance. If you want to go out and get a burger with friends, this is one way to do it.
But meat-like burgers are not equal to kale, sweet potatoes, quinoa, and other whole foods.
The same is true of pastas, breads, and baked goods that are fortified with pea, lentil, and other plant protein sources.
These options are great for people who lead busy, complex lives—and especially helpful when used as a substitute for less healthy, more highly-refined options. But they’re not a substitute for real, whole foods like broccoli.
Whether the Impossible Burger is right for your clients depends a lot on their values and where they are in their nutritional journey.
If clients want to give up meat for spiritual reasons (for example, they can’t stand the thought of killing an animal), but aren’t ready to embrace a diet rich in tofu, beans, lentils, and greens, protein-enriched meat-free substitutes may be a good way to help them align their eating choices with their values.
Isn’t meat the best source of iron—not to mention a lot of other nutrients?
Meat eaters sometimes argue that one of the cons of a vegetarian diet is this: Without meat, it’s harder to consume enough protein and certain minerals.
And there may be some truth to it.
Meat, poultry, and fish come packed with several nutrients we all need for optimal health and well-being, including protein, B vitamins, iron, zinc, and several other minerals.
When compared to meat, plants often contain much lower amounts of those important nutrients. And in the case of minerals like iron and zinc, animal sources are more readily absorbed than plant sources.
Remember that study out of Belgium that found vegans had a healthier overall dietary pattern than meat-eaters? The same study found that many fully plant-based eaters were deficient in calcium.1
Compared to other groups, fully plant-based eaters also took in the lowest amounts of protein.
Plus, they ran a higher risk of other nutrient deficiencies, such as vitamin B12, vitamin D, iodine, iron, zinc, and omega-3 fats (specifically EPA and DHA).
Is this proof that everyone should eat at least some meat?
Not really. It just means that fully plant-based eaters must work harder to include those nutrients in their diets (or take a supplement in the case of B12).
This is true for any diet of exclusion, by the way. The more foods someone excludes, the harder they have to work to include all of the nutrients they need for good health.
The Pros and Cons of Vegetarian Diets
Vegetarian diets make it easier to reduce disease risk as well as carbon emissions, but harder to consume enough protein, along with a host of other nutrients. This is especially true if someone is fully plant-based or vegan. If your client is fully plant-based, work with them to make sure they’re getting these nutrients.
Protein: Seitan, tempeh, tofu, edamame, lentils, and beans. You might also consider adding a plant-based protein powder
Calcium: Dark leafy greens, beans, nuts, seeds, calcium-set tofu, fortified plant milks
Vitamin B12: A B12 supplement
Omega-3 fats: Flax seeds, chia seeds, hemp seeds, walnuts, dark leafy greens, cruciferous vegetables, and/or algae supplements
Iodine: Kelp, sea vegetables, asparagus, dark leafy greens, and/or iodized salt
Iron: Beans, lentils, dark leafy greens, seeds, nuts and fortified foods
Vitamin D: Mushrooms exposed to ultraviolet light, fortified plant milks, and sun exposure
Zinc: Tofu, tempeh, beans, lentils, whole grains, nuts, and seeds
To help you consume enough of these nutrients each day, as part of your overall intake, aim for at least:
- 3 palm-sized portions of protein-rich plant foods,
- 1 fist-sized portion of dark leafy greens,
- 1-2 cupped handfuls of beans*
- 1-2 thumb-sized portions of nuts and/or seeds
* Only need 1 portion as a carb source if also using beans as a daily protein source.
But this plant-based influencer started eating meat—and she says she feels great. Doesn’t that prove something?
Maybe you’ve read about Alyce Parker, a formerly fully plant-based video blogger, who tried the carnivore diet (which includes only meat, dairy, fish, and eggs) for one month. She says she ended the month leaner, stronger, and more mentally focused.
Here’s the thing. You don’t have to search the Internet too long to find a story in the reverse.
A while back, for example, John Berardi, PhD, the co-founder of PN, tried a nearly vegan diet for a month to see how it affected his ability to gain muscle.
During his veggie challenge, he gained nearly 5 pounds of lean body mass.
So what’s going on? How could one person reach their goals by switching to a meat-heavy diet and another do so by giving up meat?
One or more of the following may be going on:
Dietary challenges tend to make people more aware of their behavior.
And awareness provides fertile ground for healthy habits.
New eating patterns require shopping for, preparing, and consuming new foods and recipes. This calls for energy and focus, so people invariably pay more attention to what and how much they eat.
An interesting study bears this out. Researchers asked habitual breakfast skippers to eat three meals a day and habitual breakfast eaters to skip breakfast and eat just two.
Other groups continued breakfast as usual—either skipping it (if they didn’t eat it to begin with) or eating it (if they were already breakfast enthusiasts).
After 12 weeks, the study participants who changed their breakfast habits—going from eating it to skipping it or skipping it to eating it—lost 2 to 6 more pounds than people who didn’t change their morning habits.
Whether or not people ate breakfast mattered less than whether they’d recently changed their behavior and become more aware of their intake.15
Dietary changes may fix mild deficiencies.
People who follow restrictive eating patterns, whether they’re fully plant-based or carnivore, run the risk of nutritional deficiencies.
By switching to a different, just as restrictive eating pattern, people may fix one deficiency—but eventually cause another.
Dietary changes may solve subtle intolerances.
Fully plant-based eaters, for example, who have trouble digesting lectins (a type of plant protein that resists digestion) will probably feel better on a meat-only diet.
But they could also potentially solve the problem without any meat—just by soaking and rinsing beans (which helps to remove lectins). Or by eating some meat and fewer lectin-rich foods.
Finally, the placebo effect is powerful.
When we believe in a treatment, our brains can trigger healing—even if the treatment is fake or a sham (such as a sugar pill). For this reason, as long as someone believes in a dietary change, that change has the potential to help them feel more energized and focused.
Bottom line: Any eating pattern can be healthy or unhealthy.
Someone can technically follow a fully-plant based diet without eating any actual whole plants.
For example, all of the following highly refined foods are meat-free: snack chips, fries, sweets, sugary breakfast cereals, toaster pastries, soft drinks, and so on. And meat-eaters might also include similar foods.
Vegetarian and carnivore diets only indicate what people eliminate—and not what people include.
Whether someone is on the carnivore diet, the keto diet, the Mediterranean diet, or a fully plant-based diet, the pillars of good health remain the same.
If you have strong feelings about certain eating patterns (for example, maybe you’re an evangelical vegetarian or Paleo follower), try to put those feelings aside so you can zero in on your client’s values and needs—rather than an eating pattern they think they “should” follow.
What you might find is that most clients truly don’t care about extreme eating measures like giving up meat or giving up carbs. They just want to get healthier, leaner, and fitter—and they don’t care what eating pattern gets them there.
How do we know this?
Data.
Each month, roughly 70,000 people use our free nutrition calculator. They tell us what kind of an eating pattern they want to follow, and our calculator then provides them with an eating plan—with hand portions and macros—that matches their preferred eating style. We give options for just about everything, including plant-based eating and keto.
What eating pattern do most people pick?
The “eat anything” pattern. In fact, a full two-thirds of users choose this option, with the remaining third spread across the other five options.
In other words, they don’t particularly care what they eat as long as it helps them reach their goals. Interestingly, of the many options we list, people choose fully plant-based and keto diets the least.
So rather than fixating on a “best” diet, help clients align their eating choices with their goals and values.
Ask questions like: What are your goals? What is your life like right now? What skills do you already have (can you soak beans and eat hummus and veggie wraps)? What are the foods you like to eat that make you feel good?
Encourage clients to replace what they remove.
The more foods on someone’s “don’t eat” list, the harder they must work to replace what they’re not eating.
For fully plant-based eaters, that means replacing animal protein with plant proteins found in seitan, tofu, tempeh, beans, and pulses.
For Paleo, that means replacing grains and dairy with vegetables, fruits, and sweet potatoes.
For keto eaters, that means replacing all carbs with vegetables and healthy fats like extra virgin olive oil, nuts and avocado.
Don’t just offer advice on what to eat. Spend time on how.
At Precision Nutrition, we encourage people to savor meals, eat slowly, and pay attention to internal feelings of hunger and fullness. We’ve found that these core practices alone can drive major transformation—and may be even more important than the food people put on their plates.
(Learn more about the benefits of eating slowly.)
Help them focus on being better, not perfect.
Think of nutrition as a spectrum that ranges from zero nutrition (chips, sweets, and highly refined foods) to stellar nutrition (all whole foods).
Most of us fall somewhere between those two extremes—and that’s okay, even preferred. After all, we see huge gains in health when we go from zero nutrition to average or above average.
But eventually, we experience diminishing returns.
The difference between a mostly whole foods diet and a 100 percent whole foods diet? Marginal.
So rather than aiming for perfect, it’s more realistic to try to eat a little better than you are now.
For good health, a little better for most people involves eating more minimally-processed whole foods, especially more vegetables and more protein (whether from animal or plant foods).
If your clients eat carbs, they’ll want to shift toward higher-quality options like:
- fruit
- whole grains
- beans
- legumes
- starchy tubers (such as yams and potatoes)
If they consume added fats, they can challenge themselves to showcase healthier choices such as:
- avocados
- nuts
- seeds
- olives and olive oil
Depending on the person, that might involve adding spinach to a morning omelet, adding grilled chicken to their usual lunch salad, snacking on fruit, or ordering a sandwich with guac instead of mayo.
These might sound like small actions—and that’s precisely the point. Unlike huge dietary overhauls, it’s these small, accessible, and sustainable actions that truly lead to lasting change.
More than 100,000 clients have taught us:
Consistent small actions, repeated over time, add up to big results.
And here’s the beautiful part: When you zero in on these smaller, more accessible practices, you’ll stop locking horns with clients whose beliefs fall on the opposite side of the meat vs. meat-free debate as your own.
Instead, you can work together to build universal skills and actions that everyone needs—more sleep, eating slowly, more veggies—whether they eat meat or not.
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
- Clarys P, Deliens T, Huybrechts I, Deriemaeker P, Vanaelst B, De Keyzer W, et al. Comparison of nutritional quality of the vegan, vegetarian, semi-vegetarian, pesco-vegetarian and omnivorous diet. Nutrients. 2014 Mar 24;6(3):1318–32.
- Rizzo NS, Sabaté J, Jaceldo-Siegl K, Fraser GE. Vegetarian dietary patterns are associated with a lower risk of metabolic syndrome: the adventist health study 2. Diabetes Care. 2011 May;34(5):1225–7.
- Lee-Kwan SH, Moore LV, Blanck HM, Harris DM, Galuska D. Disparities in State-Specific Adult Fruit and Vegetable Consumption – United States, 2015. MMWR Morb Mortal Wkly Rep. 2017 Nov 17;66(45):1241–7.
- Martínez Steele E, Baraldi LG, Louzada ML da C, Moubarac J-C, Mozaffarian D, Monteiro CA. Ultra-processed foods and added sugars in the US diet: evidence from a nationally representative cross-sectional study. BMJ Open. 2016 Mar 9;6(3):e009892.
- Bradbury KE, Murphy N, Key TJ. Diet and colorectal cancer in UK Biobank: a prospective study. Int J Epidemiol [Internet]. 2019 Apr 17; Available from: http://dx.doi.org/10.1093/ije/dyz064
- Murray CJL, Atkinson C, Bhalla K, Birbeck G, Burstein R, Chou D, et al. The state of US health, 1990-2010: burden of diseases, injuries, and risk factors. JAMA. 2013 Aug 14;310(6):591–608.
- Jägerstad M, Skog K. Genotoxicity of heat-processed foods. Mutat Res. 2005 Jul 1;574(1-2):156–72.
- Cross AJ, Sinha R. Meat-related mutagens/carcinogens in the etiology of colorectal cancer. Environ Mol Mutagen. 2004;44(1):44–55.
- Bouvard V, Loomis D, Guyton KZ, Grosse Y, Ghissassi FE, Benbrahim-Tallaa L, et al. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015 Dec;16(16):1599–600.
- Han MA, Zeraatkar D, Guyatt GH, Vernooij RWM, El Dib R, Zhang Y, et al. Reduction of Red and Processed Meat Intake and Cancer Mortality and Incidence: A Systematic Review and Meta-analysis of Cohort Studies. Ann Intern Med [Internet]. 2019 Oct 1; Available from: http://dx.doi.org/10.7326/M19-0699
- Bradbury KE, Murphy N, Key TJ. Diet and colorectal cancer in UK Biobank: a prospective study. Int J Epidemiol [Internet]. 2019 Apr 17; Available from: http://dx.doi.org/10.1093/ije/dyz064
- Gardner CD, Hartle JC, Garrett RD, Offringa LC, Wasserman AS. Maximizing the intersection of human health and the health of the environment with regard to the amount and type of protein produced and consumed in the United States. Nutr Rev. 2019 Apr 1;77(4):197–215.
- Kim BF, Santo RE, Scatterday AP, Fry JP, Synk CM, Cebron SR, et al. Country-specific dietary shifts to mitigate climate and water crises. Glob Environ Change. 2019 Aug 7;101926.
- Liu C, Cutforth H, Chai Q, Gan Y. Farming tactics to reduce the carbon footprint of crop cultivation in semiarid areas. A review. Agron Sustain Dev. 2016 Nov 16;36(4):69.
- Schlundt DG, Hill JO, Sbrocco T, Pope-Cordle J, Sharp T. The role of breakfast in the treatment of obesity: a randomized clinical trial. Am J Clin Nutr. 1992 Mar;55(3):645–51.
If you’re a coach, or you want to be…
Learning how to coach clients, patients, friends, or family members through healthy eating and lifestyle changes—in a way that’s personalized for their unique body, goals, and personal preferences—is both an art and a science.
If you’d like to learn more about both, consider the Precision Nutrition Level 1 Certification. The next group kicks off shortly.
What’s it all about?
The Precision Nutrition Level 1 Certification is the world’s most respected nutrition education program. It gives you the knowledge, systems, and tools you need to really understand how food influences a person’s health and fitness. Plus the ability to turn that knowledge into a thriving coaching practice.
Developed over 15 years, and proven with over 100,000 clients and patients, the Level 1 curriculum stands alone as the authority on the science of nutrition and the art of coaching.
Whether you’re already mid-career, or just starting out, the Level 1 Certification is your springboard to a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results.
[Of course, if you’re already a student or graduate of the Level 1 Certification, check out our Level 2 Certification Master Class. It’s an exclusive, year-long mentorship designed for elite professionals looking to master the art of coaching and be part of the top 1% of health and fitness coaches in the world.]
Interested? Add your name to the presale list. You’ll save up to 30% and secure your spot 24 hours before everyone else.
We’ll be opening up spots in our next Precision Nutrition Level 1 Certification on Wednesday, April 8th, 2020.
If you want to find out more, we’ve set up the following presale list, which gives you two advantages.
- Pay less than everyone else. We like to reward people who are eager to boost their credentials and are ready to commit to getting the education they need. So we’re offering a discount of up to 30% off the general price when you sign up for the presale list.
- Sign up 24 hours before the general public and increase your chances of getting a spot. We only open the certification program twice per year. Due to high demand, spots in the program are limited and have historically sold out in a matter of hours. But when you sign up for the presale list, we’ll give you the opportunity to register a full 24 hours before anyone else.
If you’re ready for a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results… this is your chance to see what the world’s top professional nutrition coaching system can do for you.
The post The modern diet dilemma: Is it better to… eat meat? Go vegan? Something in between? The truth about what’s right for you. appeared first on Precision Nutrition.
Source: Health1
When it comes to fat loss and muscle gain, everyone wants Insta-worthy after photos… right now. But understanding what’s realistic can be the difference between achieving amazing results and giving up altogether. How fast can a client lose fat? What’s the upper limit of muscle gain? And how do you figure out a rate of progress that your client can not only achieve but sustain? We have the numbers—and your coaching game plan.
+++
Imagine you have two new clients.
Courtney—a 34-year old female—wants to lose the extra 30 pounds she’s packed on since college.
Jose—a 27-year old male—wants to add 15 pounds of muscle to his frame.
Like many clients, they both say they’re ready to do whatever it takes.
Knowing all this, how long should it take each to achieve their goals?
A. 3 months
B. 6 months
C. 1 year
Answer: It depends.
Each option may be doable, but all three come with tradeoffs. And unless you help Courtney and Jose fully understand this—and set their expectations appropriately—they’re likely to end up disappointed.
Sound familiar?
When it comes to losing fat or gaining muscle, people are often frustrated by what they think are “poor” or “mediocre” results.
Not due to lack of progress, but because:
- They started with unrealistic expectations
- They couldn’t sustain their initial rate of progress
- All of the above
It doesn’t have to be this way.
In this article, we’ll share what realistic rates of both fat loss and muscle gain look like, based on a combination of clinical evidence and our work with over 100,000 clients.1, 2
More importantly, we’ll show you how to determine a rate of progress that’s right for your client (or even yourself). For results that meet expectations—every single time.
But… if you want to jump right to the numbers, click the links below:
Otherwise, keep reading (the details matter) for the complete story.
Results not typical… or are they?
Let’s say Courtney lost six pounds of body fat in your first four weeks together. Yet she was disappointed in her “lack” of progress.
From our standpoint, her progress was fantastic.
Over six months, maintaining that rate of progress would lead to a 40-pound fat loss.
That could be life-changing for some. For others, it might be way more than they’d even want to lose. (In fact, it’s more than Courtney wanted to lose.)
Yet all too often, the client thinks they’re failing. Because six pounds in four weeks doesn’t feel like a lot.
This is likely because they expected extremely rapid results. Perhaps they hoped to quickly look like they did 15 years ago or have the body comp of a magazine cover model… by next month’s vacation.
Now, most people would readily admit that expecting to lose 15 pounds of fat or gain 10 pounds of muscle in two weeks is unrealistic. (The same goes for correcting serious blood lipid issues or knocking a half-second off their 40-yard dash time.)
But subconsciously, they still want to believe these results are not only possible but likely. After all, they’ve seen The Biggest Loser.
Your job: Set achievable expectations from day one.
Understand the true goal and what success looks like.
This starts by finding out what your client ultimately hopes to achieve.
- Do they want to lose a few pounds and get healthier?
- Do they want to look fit in clothes?
- Do they want to pack on 15 pounds of muscle?
- Do they want to be “shredded,” with visible abs?
Make sure you have a shared understanding of what they’re envisioning.
You want to be in complete agreement. So ask more questions and dig deeper.
‣ If they say they want to lose 20 pounds, what do they picture? Many people underestimate how much fat they’d have to lose to achieve a certain body composition. They might think they need to drop 20 pounds, when in fact, it’s more like 40.
‣ If they want to “get healthier,” how will they know when they arrive? Are they picturing better blood work, and if so, what specific measures are they concerned about?
‣ If they want to gain muscle, are they okay gaining some fat, too? Do they see themselves as The Rock, or just a slightly bigger version of themselves?
‣ If they want to “look muscular,” getting leaner might help them achieve that goal faster. As the saying goes, “Losing fat is the fastest way to look bigger.”
‣ If they want a six-pack, are they prepared for all that entails? Achieving this type of physique often requires a greater amount of exercise, a more restrictive diet, and a less flexible lifestyle. What’s more, if they’ve been over-fat for a long time, it could come with some loose skin.
Walking clients through their desired scenario can help them better choose a path based on what’s most important to them.
Make sure the tradeoffs are crystal clear.
Simply put: You want your client to know what they’re getting into.
An effective way to do this: Put your client’s desired outcome on a continuum next to two (or more) other outcomes.
If you want to highlight how unlikely or difficult the goal will be, show what it’ll take to achieve two easier goals.
You could say: “Here are the tradeoffs that you’ll need to make to reach your goal, and for comparison, here’s what two other outcomes might require. Do those tradeoffs feel acceptable to you?”
On the other hand, if you want to give the client more confidence, you might sandwich their goal between one that’s easier and one that’s harder.
You could say: “There’s no doubt your goal will be a challenge, but at least you can eat dessert most days and still achieve it. What do you think about that?”
Here’s an example of how this might look. The illustrations that follow show the tradeoffs typically required to achieve three different levels of body fat.
As you can see, the lower your body fat percentage goal, the greater the commitment that’s required. (For a deeper dive on this topic, read: The Cost of Getting Lean.)
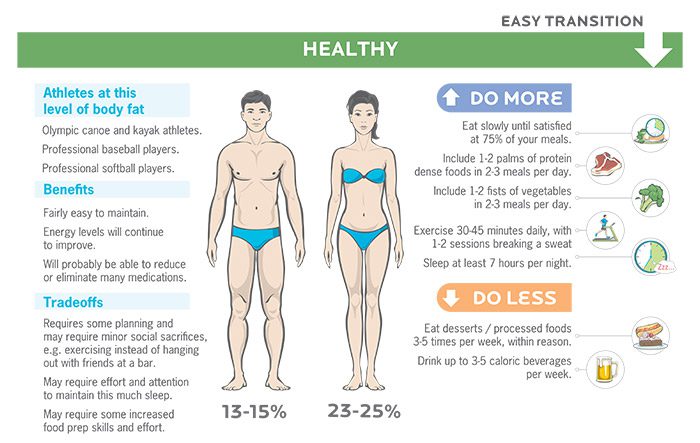
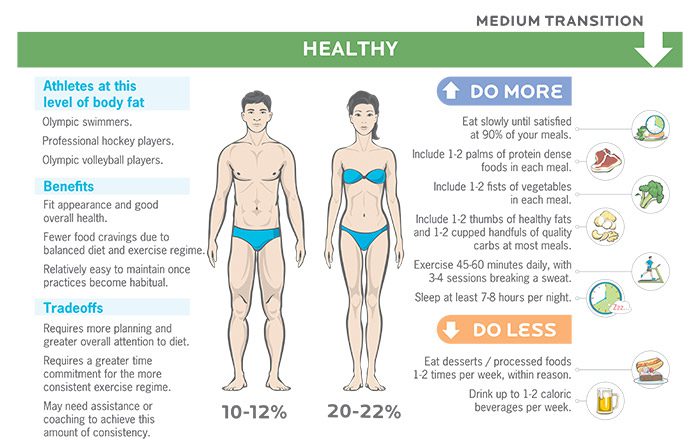

To ensure both you and your client understand what they want to achieve, and what they’re willing (and not willing) to do to achieve it, download and use the Want-Willing-Won’t Worksheet.
Now it’s time to talk timelines. We’ll cover realistic rates of fat loss first, followed by realistic rates of muscle loss.
Realistic rates of fat loss.
How fast you can lose body fat depends on how consistently you can, or want to, follow the guidelines you’re given.
Realistic rates of fat loss per week
| Progress | % Body Weight | Men | Women |
|---|---|---|---|
| Extreme | 1-1.5% body weight | ~2-3 lb | ~1.65-2.5 lb |
| Reasonable | 0.5-1% body weight | ~1-2 lb | ~0.8-1.65 lb |
| Comfortable | <0.5% body weight | ~<1 lb | ~<0.8 lb |
Here’s how to quantify each of these categories:
Extreme: Requires about 90 to 100 percent consistency.
Reasonable: Requires about 70 to 85 percent consistency.
Comfortable: Requires about 50 to 65 percent consistency.
(Note: You could also create a comfortable rate of progress in which you’re highly consistent. Your initial action plan would simply require you to make fewer changes than what’d be necessary to achieve reasonable or extreme rates of progress.)
Clearly, the more consistent you are, the faster your progress, and the more fat you’ll lose.
It’s also important to realize that fat loss is rarely linear. It fluctuates from day to day and week to week. The goal is to see an overall trend downward over time.
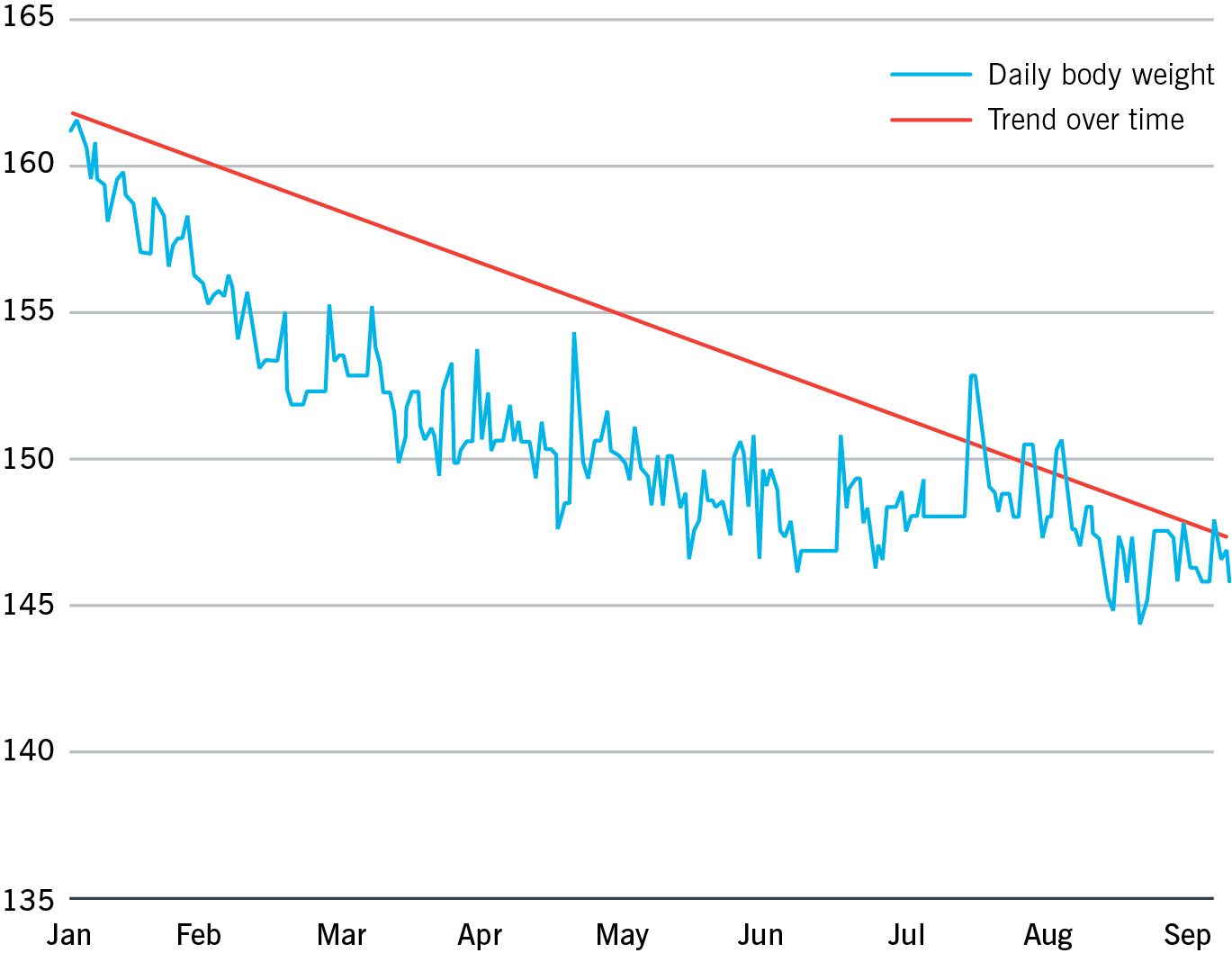
But… fat loss is often fastest when:
- You’re first starting out
- You have more body fat to lose
Why? Suppose you normally eat 3,500 calories per day and are maintaining your body weight. If you suddenly start eating 2,000 calories a day, you’ve created a massive deficit of 1,500 calories. That’ll lead to rapid weight loss.
Once you start to lose body weight, however, this deficit becomes smaller and smaller, slowing fat loss. (Because a smaller body requires fewer calories.)
As this process continues, your metabolism adapts, lowering your calorie needs even more than what you’d expect from the weight loss alone. You’ll also become more efficient at exercising, reducing the number of calories you burn through movement.
And if that’s not enough, you might even exercise less frequently and intensely because you now have less energy coming in. (To learn more, read: How your metabolism adapts as you lose weight.)
The upshot:
The leaner you become, the slower your rate of fat loss, and the more plateaus you experience.
This is normal. And helping clients understand this leads to better progress.
That’s because they’ll be less likely to throw in the towel when fat loss stalls for a week or two. Instead, they’ll understand it’s a normal part of the journey.
Encourage clients to think of fat loss like a long road trip. If they know going in that they’ll have to stop for food and bathroom breaks, and that they’ll probably experience some traffic jams and construction detours, they won’t be dismayed when those things happen. (Because they will. That’s life.)
It won’t always be smooth sailing. Coach them to expect disruptions ahead of time. This mental preparation will be valuable down the road.
Realistic rates of muscle gain.
The ability to gain muscle is dependent on age, biological sex, genetics, and consistency with food intake, along with resistance training experience, intensity, frequency, style, volume, and more.
Realistic rates of muscle gain per month
| Fitness level | Men | Women | ||
|---|---|---|---|---|
| Beginner | 1-1.5% body weight |
~1.5-2.5 lb | 0.5-0.75% body weight |
~0.65-1 lb |
| Intermediate | 0.5-0.75% body weight |
~0.75-1.25 lb | 0.25-0.375% body weight |
~0.325-0.5 lb |
| Advanced | 0.25-0.375% body weight |
~0.375-0.625 lb | 0.125-0.1875% body weight |
~0.1625-0.25 lb |
Much like fat loss, muscle gain is often not linear. Progress seems to come in fits and spurts, especially after the first year of dedicated training.
It’s not uncommon to see young men gain 15 to 25 pounds of muscle in their first year of dedicated training (beginner), and another 10 to 15 pounds in their second year (intermediate).
Young women can see gains of 8 to 12 pounds of muscle in their first year of dedicated training (beginner), along with another 4 to 6 pounds in their second year (intermediate).
After the first three or so years of dedicated training (advanced), it often takes years of persistent effort to see incremental gains.
So over the course of a lifting career, men have the potential to gain about 40 to 50 pounds of muscle, and women have the potential to gain about 20 to 25 pounds of muscle. (Depending on height, bone structure, and genetics—and without the help of performance-enhancing drugs.)
For the realistic rates of muscle gain shown here, the emphasis is on “young” men and women under the age of 30. Testosterone and other sex hormones are higher during this time of life, as is cellular turnover and overall recovery capacity. All are key factors for muscle growth.
Older men and women usually add less muscle and/or at a slower rate, due to changes in these variables.
Can you still gain significant muscle after your 20s? Yes, but for the most part, this depends on whether or not you still have a fair amount of room to reach your 40 to 50 pound (men) or 20 to 25 pound (women) potential.
Identify a likely rate of fat loss or muscle gain for each individual.
Consider the realistic rates of fat loss and muscle gain the upper limit of what can be achieved in a given time frame. Now you have to adjust that number, based on the person and conditions you’re working with.
This is where the art of coaching really comes in.
The rate of body composition changes can be affected by the following factors.
Factors that make fat loss harder or easier
| What makes fat loss harder | What makes fat loss easier | |
|---|---|---|
| Age | Being older* | Being younger |
| Sex | Being female | Being male |
| Current body size | Being smaller | Being heavier |
| Current body composition | Being relatively lean | Having more body fat |
| Current activity level | Little to no activity | High levels of activity |
| Current activity type | Doing excessive cardio without other types of activity | Having a well-rounded exercise regimen |
| Consistency | Being inconsistent | Being consistent (>80%) |
| Recovery | Sleeping less than 7 hours most nights | Sleeping at least 7-8 hours most nights |
| Stress | Excessive stress or perception of excessive stress | Appropriate stress levels or perception of appropriate stress |
| Hormones | Leptin-resistance / low leptin Insulin-resistance |
Hormones in healthy ranges |
| Medication | Birth control Corticosteroids Antidepressants |
Xenical / Alli Belviq Qsymia Contrave Saxenda PEDs |
| Health status | Menopause Hypothyroidism PCOS Cushing’s syndrome Depression |
Clean bill of health |
*Fat loss can and does occur at any age. The reasons it can be harder for older folks may be more age-related (health status, medications, mobility) as opposed to age-dependent.
Factors that make muscle gain harder or easier
| What makes muscle gain harder | What makes muscle gain easier | |
|---|---|---|
| Age | Being older (>40) | Being younger (<30) |
| Sex | Being female | Being male |
| Current body size | Having a small frame / bone structure | Having a large frame / bone structure |
| Current body composition | Having more body fat | Being relatively lean |
| Current activity level | Little to no activity | Moderate levels of activity |
| Current activity type | Inadequate resistance training / excessive cardio | Resistance training |
| Consistency | Being inconsistent | Being consistent (>80%) |
| Recovery | Sleeping less than 7 hours most nights | Sleeping at least 7-8 hours most nights |
| Stress | Excessive stress or perception of excessive stress | Appropriate stress levels or perception of appropriate stress |
| Hormones | High cortisol | Hormones in healthy ranges |
| Medication | Thyroid drugs ADHD drugs Acne medication |
PEDs |
| Health status | IBD Gastroparesis Hyperthyroidism Depression |
Clean bill of health |
These are by no means exhaustive lists, but are good examples of how additional factors can impact an individual’s rate of progress.
You also need to account for what else is happening in a person’s life.
Will your client improve at a consistent rate or might there be periods where progress slows?
For example, if they’re an accountant, you may need to adjust expectations during tax season. During the holidays, the goal might just be to maintain current progress, then aim to make further progress after the holidays have passed. And what about upcoming vacations or other planned breaks?
You can’t foresee every issue, but you can plan for what you know.
For these periods, ask your client how little improvement they’re willing to accept and how long they expect these periods to last. Together, you can incorporate that information into the timeline.
Once you have a good idea of where they want to go and how fast they could get there, it’s time to fully review what’s required. Is your client “ready, willing, and able” to do what it takes?
You can test this by using the Ready, Willing, and Able Worksheet.
This is where you find out how realistic the rates of progress truly are, based on the action plan you create with your client.
Now that the next steps are in front of them, how confident are they about following through? Remember: The key to success is consistency. (Learn more: How to create a plan clients can do consistently.)
If your client isn’t ready, willing, able to follow through consistently, that’s okay. You’ll simply need to adjust their action plan. And that also means adjusting their expectations.
But that’s good news: With this approach, you’ll both be on the same page from the get-go.
Revisit and re-calibrate expectations as data accumulate.
No one can perfectly predict a client’s rate of progress. This exercise simply gives you a way to measure if your client is moving in the right direction at their desired rate, or if their outcomes are falling short of expectations.
In general, you should monitor results for two weeks before recommending your client adjusts their food intake or action plan.
And as they become more advanced, or progress closer to their final goal, it may take a full four weeks to see if their intake is working. Give it an appropriate amount of time before considering further adjustments.
As you gather data, and choose next actions based on that data, continually review and revise your clients’ plans and expectations. (Click here to download a printable guide that lets you reference the information below at a glance.)
Not losing fat within realistic parameters?
Decrease your client’s intake by about 250 calories a day, by cutting out about 25 to 50 grams of carbs and/or 7 to 15 grams of fat. Or simply remove 1 to 2 cupped handfuls of carbs and/or 1 to 2 thumbs of fats from their daily intake. (That’s 2 to 3 total portions of carbs and fats, combined.)
Not gaining muscle within realistic parameters?
Increase your client’s intake by about 250 calories a day, by adding 25 to 50 grams of carbs and/or 7 to 15 grams of fats. Or simply add 1 to 2 cupped handfuls of carbs and/or 1 to 2 thumbs of fats to your daily intake. (That’s 2 to 3 total portions of carbs and fats, combined.)
Losing too much lean mass when losing weight?
Increase your client’s daily protein intake by about 25 grams. Or simply add 1 extra palm of protein to your daily intake.
Gaining too much fat when adding muscle?
Increase your client’s daily protein intake by about 25 grams, and decrease their daily carb intake by about 25 to 50 grams and/or fat intake by about 7 to 15 grams.
Or simply add 1 extra palm of protein to your daily intake, and remove 1 to 2 cupped handfuls of carbs and/or 1 to 2 thumbs of fats from your daily intake. (That’s 2 to 3 total portions of carbs and fats, combined.)
Not recovering from tough workouts or competitions?
Use these four steps:
Step 1. Review your overall daily energy intake. If you’re cutting calories stringently to lose fat or weight, consider increasing energy intake by 100 to 200 calories so that you’re eating at just a slight deficit.
Step 2. Review your total daily protein intake. Just adding 25 more grams or 1 more palm of protein per day can make a difference.
Step 3. Review your total daily carbohydrate intake. You may need more than you’re getting, particularly right after training sessions or games/competitions. A good start: Add 25 to 50 grams (or 1 to 2 cupped handfuls of carbs) to your daily intake.
Step 4. Review your total daily fat intake, particularly your intake of essential fatty acids. If you’re noticing a lot of inflammation, you might benefit from increasing your intake of “Eat More” fat sources, and decreasing your intake of “Eat Less” fat sources. (See a variety of both sources in the article: What Foods Should I Eat?)
Let the facts guide you.
Clients may progress faster or slower than you expected, or they may encounter unexpected challenges (such as an injury or illness).
This is absolutely okay. Base predictions and expectations on known data, not imagination, hopes, or assumptions.
As the great psychotherapist Carl Rogers once said, “The facts are friendly.” No matter what happens, consider this calibration an essential and valuable part of helping you become a more accurate and evidence-driven coach.
This type of outcome-based decision making is a powerful coaching tool for helping clients see how their actions lead to progress and results.
Remember, numbers aren’t the only way to measure progress.
It can be tempting to focus only on quantitative data: body fat percentage, inches lost, the number on the scale. But progress is just as much about subjective measures, such as:
- Showing up and making any effort, no matter how small
- Tiny actions that are just a little bit better than before
- Feeling more at ease with food
- Daily wins, like having breakfast on your busiest morning
- Having more energy and vitality
- Getting stronger and/or fitter
- Feeling more confident in one’s body or sense of self
- And more
Make sure your client understands how far they’ve come, no matter what the numbers show. Regularly pointing out the bright spots—especially in behaviors, actions, and mindset—gives the client positive feedback they can build on.
The Looking Back, Looking Ahead Worksheet is often super helpful in this regard. It’s a way for clients to see how far they’ve come, which can boost their confidence and keep them motivated. It can also help them proactively work around potential obstacles.
As we say here at Precision Nutrition:
It’s about progress, not perfection.
And whether your clients want to lose fat or gain muscle, that may be the most important expectation you can set.
jQuery(document).ready(function(){
jQuery(“#references_link”).click(function(){
jQuery(“#references_holder”).show();
jQuery(“#references_link”).parent().hide();
});
});
References
Click here to view the information sources referenced in this article.
1. NHLBI Obesity Education Initiative Expert Panel on the Identification, Evaluation, Treatment of Obesity in Adults (US). Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. National Heart, Lung, and Blood Institute; 1998.
2. Helms ER, Aragon AA, Fitschen PJ. Evidence-based recommendations for natural bodybuilding contest preparation: nutrition and supplementation. J Int Soc Sports Nutr. 2014 May 12;11:20.
If you’re a coach, or you want to be…
Learning how to coach clients, patients, friends, or family members through healthy eating and lifestyle changes—in a way that sets realistic expectations and is personalized for their unique body, goals, and preferences—is both an art and a science.
If you’d like to learn more about both, consider the Precision Nutrition Level 1 Certification. The next group kicks off shortly.
What’s it all about?
The Precision Nutrition Level 1 Certification is the world’s most respected nutrition education program. It gives you the knowledge, systems, and tools you need to really understand how food influences a person’s health and fitness. Plus the ability to turn that knowledge into a thriving coaching practice.
Developed over 15 years, and proven with over 100,000 clients and patients, the Level 1 curriculum stands alone as the authority on the science of nutrition and the art of coaching.
Whether you’re already mid-career, or just starting out, the Level 1 Certification is your springboard to a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results.
[Of course, if you’re already a student or graduate of the Level 1 Certification, check out our Level 2 Certification Master Class. It’s an exclusive, year-long mentorship designed for elite professionals looking to master the art of coaching and be part of the top 1% of health and fitness coaches in the world.]
Interested? Add your name to the presale list. You’ll save up to 30% and secure your spot 24 hours before everyone else.
We’ll be opening up spots in our next Precision Nutrition Level 1 Certification on Wednesday, April 8th, 2020.
If you want to find out more, we’ve set up the following presale list, which gives you two advantages.
- Pay less than everyone else. We like to reward people who are eager to boost their credentials and are ready to commit to getting the education they need. So we’re offering a discount of up to 30% off the general price when you sign up for the presale list.
- Sign up 24 hours before the general public and increase your chances of getting a spot. We only open the certification program twice per year. Due to high demand, spots in the program are limited and have historically sold out in a matter of hours. But when you sign up for the presale list, we’ll give you the opportunity to register a full 24 hours before anyone else.
If you’re ready for a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results… this is your chance to see what the world’s top professional nutrition coaching system can do for you.
The post Fat loss and muscle gain: What does realistic progress look like? appeared first on Precision Nutrition.
Source: Health1
When it comes to nutrition, there’s plenty we don’t know.
Although it may be hard to accept, the jury’s still out on red meat. On eggs. On low carb versus low fat. On Paleo versus fully plant-based.
In fact, there’s very little we can say with absolute certainty.
Science hasn’t identified one best diet or eating approach.
Because of that, you can be sure no documentary filmmaker has. No matter how compelling or convincing the movie.
(This includes filmmakers you agree with, by the way.)
So what do you do when a client—or a friend or family member—watches a trending nutrition documentary and becomes captivated with:
- nutrition advice that contradicts what you’ve been telling them?
- questionable eating methods you believe will set them back?
- an extreme diet you’re pretty darn sure will fail?
First, take a breath. (Or two.)
Next, understand that, in most cases, you can’t “prove” anyone wrong.
More importantly: You shouldn’t even try.
There’s a much healthier and more effective approach for your clients, your business, and your sanity…
Aim to be helpful, not right.
This mindset lightens the tone of your conversations, fosters trust and appreciation, and allows you to ultimately have greater influence. (It’ll make you more likable on social media, too.)
Admittedly, this doesn’t always feel second nature. But with practice, it can become that way.
The payoff is huge: Instead of dreading the next big nutrition documentary, you can use it to build a stronger and more productive relationship with anyone who seeks your help.
This article will show you how.
Why you don’t need to be right.
Before we get to helping clients, let’s address a big hurdle: Our deep need to be right.
The reality is this: Most nutrition debates won’t be resolved anytime soon. Probably not even in our lifetimes.
(To better understand why, read: Why nutrition science is so confusing.)
You might even think of it this way:
Scientific progress is more about being progressively less wrong than suddenly understanding some ultimate truth.
So in many ways, we’ll never really know if we’re “right.”
Accepting this can help you become a more thoughtful, open coach (and human being).
Plus, trying to prove to your client that you’re “right” interferes with your ability to develop a strong coaching relationship. It might even hinder your chances of helping them.
Because unless you ask questions to find out what resonates with your client about “Diet Fad X,” you’ll never understand what need they’re trying to meet with that approach.
That’s a missed opportunity to leverage what matters to your client to create real change. (More on why the best coaches shut up and listen in a bit.)
There’s one downside, however, with accepting that there’s often no “right” answer in nutrition: It can be unsettling.
For some coaches, nutritional uncertainty raises foundation-shaking questions, such as:
- How can you feel comfortable giving guidance based on incomplete information?
- How can you avoid a crisis of confidence when you encounter a new, exciting nutritional theory—that goes against everything you were taught?
- How can you tell the difference between evolving your coaching philosophy and getting caught up in a fad?
To help answer these questions, Craig Weller, Precision Nutrition Master Coach and resident exercise specialist, points to a fascinating research paper titled, The End of History Illusion. It provides a useful analogy for coming to terms with nutritional uncertainty.
The scientists’ findings: If you ask someone how much they’ve changed as a person in the past and how much they believe they’ll change in the future, they’ll virtually always say that most of their change is already behind them. This is true whether they’re 18 or 68.
“As humans, we tend to believe we’re already the person we’ll be for the rest of our lives, but that’s not how it actually works,” says Weller. “It’s the same in science and nutrition.”
“If we look back 150, 20, or even just 10 years ago, there were things people strongly believed to be true about nutrition that eventually were disproven or shown to be irrelevant.”
This isn’t to suggest you should ignore the current thinking and research on nutrition. It’s to emphasize uncertainty has always existed, not only in nutrition and science but in almost every aspect of life.
Even if we feel certain about something today—the love of our life, that awesome new job, a SpongeBob tattoo—we might feel very different in a decade.
So what can you do?
Focus on what you know with the highest degree of confidence in any given moment.
(We’ll cover the specifics in the next section.)
Then explore new ideas and alternative methods as experiments. Gather data, and choose the best path forward based on the outcome.
The benefit: You don’t need to be right before you start. You can use nutrition experiments to better understand what works for each individual.
This is truly customized nutrition coaching, and it keeps you open (and chill) to any approach your client wants to try.
What we (mostly) know for sure about nutrition science
If you think nutritional uncertainty causes problems for you, imagine what it’s like for clients.
“There’s a lot of contradictory information out there, causing tribalism and discord where there need not be any,” says Brian St. Pierre, MS, RD, CSCS, Precision Nutrition’s director of nutrition.
“These passionate and often conflicting messages only end up confusing people and discouraging them from getting started in the first place, since it appears that ‘no one knows what’s right anyway.’”
This is where you can help provide clarity and focus.
How? By emphasizing the importance—and effectiveness—of just a handful of very basic principles.
Despite all of the seemingly-conflicting information, there are several foundational elements that virtually everyone agrees with, says St. Pierre:
- Eat more minimally-processed whole foods and fewer highly-processed foods
- More vegetables are better than fewer vegetables
- Eating enough protein is crucial for health, performance, and body composition
- In the long-term, learning to manage your food intake based on your body’s hunger and fullness cues works better than weighing and measuring everything you eat. (Read more on this topic.)
“Make these four principles the foundation of your dietary recommendations,” says St. Pierre.
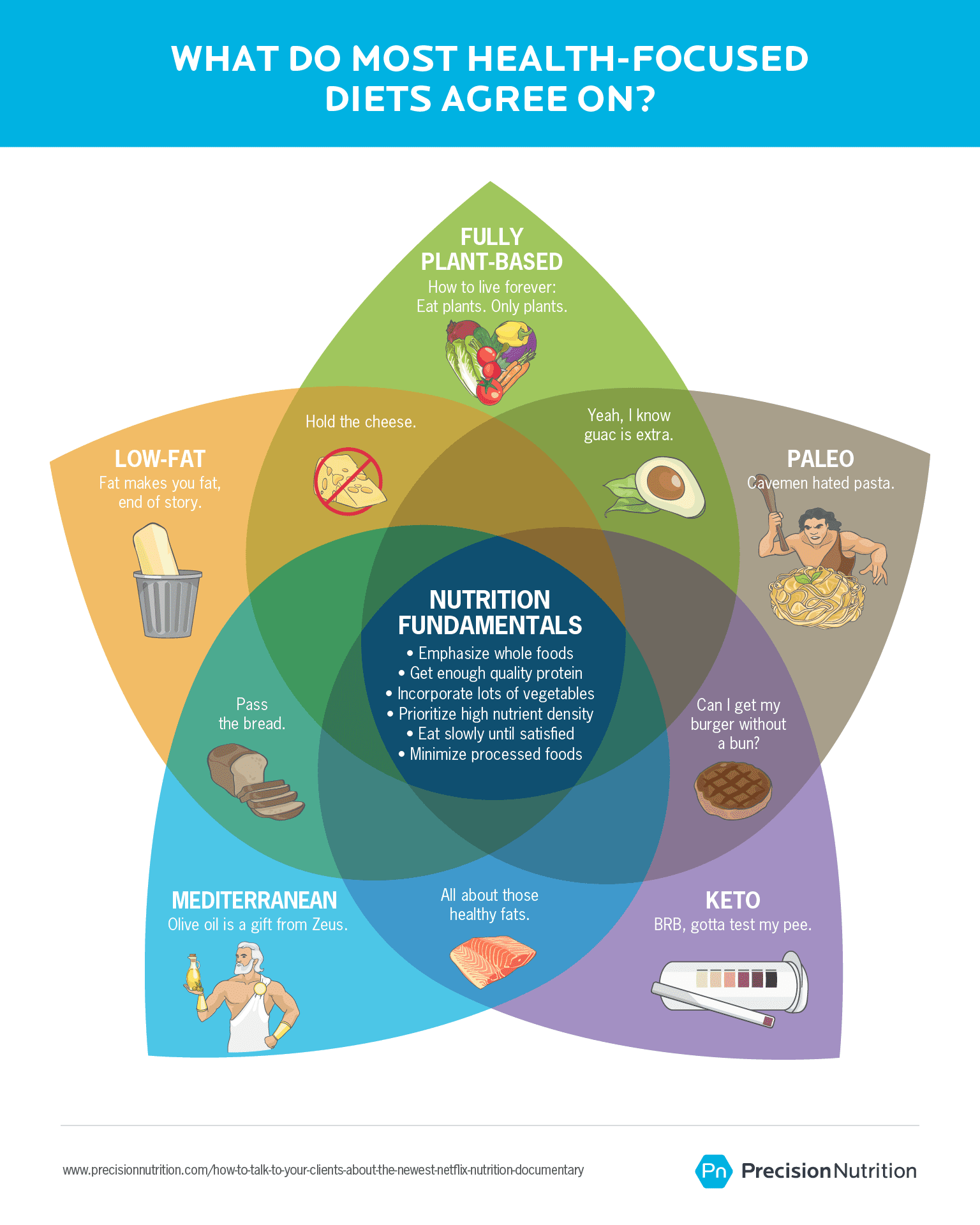
Think of the middle of the Venn diagram as the fundamentals of nutrition. These keep clients on track and help you feel confident in your advice.
And those outside sections? They aren’t life or death. Whether your client wants to eat like a caveman, give up meat forever, or make olive oil their life force is a matter of personal preference.
Ultimately, your client is the boss of how they eat.
So if they want to try something new as a result of a nutrition documentary, that’s their call.
Your role: Help them do it better.
Here’s how to do just that.
Your 5-step guide for helping clients (even if you think they might be wrong)
Step 1: Give positive feedback.
If a client is excited by a nutrition documentary, don’t tell them it’s wrong. This can feel dismissive, and it minimizes their thoughts and feelings.
Instead, do as David Burns, MD, a pioneer in the field of cognitive behavioral therapy and creator of the T.E.A.M. counseling method says: “Find the truth in what they’re saying.”
One way to do that is through positive feedback, says Precision Nutrition Master Coach Kate Solovieva, MA. “This allows your client an opportunity to engage in ‘self-enhancement,’ a basic type of motivation that’s associated with both increased self-esteem and sense of control.”
These are assets when you’re helping someone improve their nutrition.
Welcome their questions, opinions, and concerns in a way that says, “What you think matters, and I want to talk about anything important to you.”
For example:
- If they ask a question, you might lead with: “I’m so glad you asked!”
- If they’re concerned about how their current habits might impact their well-being: “It’s awesome you care so much about your health!”
- If they’ve taken a keen interest in a particular documentary or nutrition topic: “I’m impressed you’re looking into nutrition in your spare time. That’s pretty cool!”
Step 2: Express curiosity.
“See if you can have a discussion about the film without explicitly stating your beliefs about it,” advises Solovieva.
So, ask lots of questions and be a good listener. Or as Solovieva says: “Practice good coaching.”
Your charge: Find out what they learned that was so intriguing (or unsettling) to them… and why.
Here are some questions that could help you learn more, and potentially help you decide (together) what to do next:
If they’re resisting what you’ve been telling them because the nutrition documentary conflicts…
- Ask this: “Can you tell me a bit more about that? Which points stood out to you? What seems like a better approach to you, and why?”
If they’re worried their current plan is taking them down the wrong path…
- Ask this: “I can understand why you’re concerned. I’m wondering if you can tell me more about how the documentary conflicts with the work we’re doing together? Is there anything specific you’d like to do differently?”
If they’re interested in implementing changes based on the nutrition documentary…
- Ask this: “What about making this change feels appealing to you? How do you think this change will benefit you? Is there anything about it that you think will be challenging?”
This approach helps show your client they’re in control. And simply knowing they’re the decision-maker—and that you’ll support their choice—gives them more confidence in your advice.
Step 3: Support, don’t judge.
No matter what, you want your client to know you’re on their side.
Let’s say they want to try an approach you wouldn’t generally recommend. For instance, depending on your views, it might be veganism, keto, or intermittent fasting. You want them to feel comfortable discussing their choice with you—so they’ll come to you if they slip up, need help, or decide to change course.
In other words, there’s no place for “I told you so” in good coaching.
Because ultimately, your client is either going to:
- Decide not to make any changes after talking it over with you.
- Make a change, realize it’s not working for them, and lean on you for help.
- Find out they actually do love vegan, keto, IF, or [insert whatever diet].
All of which are positive.
Here are some ways you can show your client that you support them no matter what they decide to do:
If they’ve already made up their mind about making a specific change…
- Say this: “That sounds like an interesting idea. Would you like suggestions on how to implement it and monitor your progress?”
If they’re not sure what to do next…
- Say this: “I can tell you’re unsure about what happens next. What are the options you’re considering? Let’s talk through them.”
If they try something new and it doesn’t work out:
- Say this: “This is great intel. Learning what doesn’t work for you is really important. What are your takeaways from this experience?”
Step 4: Collaborate on an action plan.
After you’ve listened to and understood your client’s concerns—and shown you’ll support them—it’s time to take action.
But don’t tell your client what to do. (Even if they want you to.) Instead, take what you’ve discovered and use it to guide your client.
Maybe they just want to make a small change, to find out if it would make a difference for them.
In this case, give your client options. Let’s say they want to incorporate more celery juice into their diet. They heard it could boost their health while trying to lose weight, especially if they have it on an empty stomach for breakfast.
You might present these options:
Option A: Keep everything the same. “Things are already going pretty well, so you might not even need the celery juice.”
Option B: Go for the middle path. “If you want to try incorporating celery juice, you could plan to have it a couple of mornings a week, but still eat your regular breakfast, too.”
Option C: Go all out. “You could also switch to having just celery juice for breakfast every morning. I’d want to make sure you get some high-quality protein, carbohydrates, and healthy fats at your next meal, though.”
These three choices—do nothing, do something, do the most you can possibly do—work for most any nutrition change your client may be interested in.
If the change is something that doesn’t seem risky to you—like eating more vegetables or drinking more celery juice—feel free not to offer your opinion.
If you think the “all-out” option could put your client’s health at risk, or seriously derail their progress, speak up.
You might say something like, “I personally recommend option A or B, as I’m concerned that option C could actually be detrimental to your health. But it’s not up to me. Only you can decide how we move forward.”
Now, your client could want to overhaul the way they eat entirely. But don’t panic! This is where experimentation comes in.
Step 5: Encourage your client to think like a scientist.
Self-experimentation is one of the cornerstones of the Precision Nutrition coaching program. Because every person is different, you never know exactly how a particular way of eating is going to work until you try.
Here’s how to frame an eating experiment for your client, courtesy of Krista Scott-Dixon, PhD, Precision Nutrition’s director of curriculum.
“Use words like ‘exploration,’ ‘try,’ and ‘game,’ when talking about this with clients,” says Dr. Scott-Dixon. “Say something like:
We’re going to play a little game for the next two weeks.
You’re going to be a scientist, and you’re going to collect data about yourself. Let’s come up with some indicators to track that will help us decide whether this is moving you towards or away from your goals.
Once you gather the data, we can analyze it together. We can even make some charts and PowerPoints if you want.
Then, we’ll draw conclusions and do some outcome-based decision making, just like scientists, to see what our next steps are. But you’re going to be the authority on your own experience.’”
Talking about the experiment as something scientific but fun encourages your client to put their scientist hat on. There are many benefits to working this way. It may help your client:
- detach emotionally from the outcome of the experiment
- discover something new about their relationship with food/nutrition
- put aside “the research” and become immersed in their own experience
- recognize that what works for others may not necessarily work for them
- consider other experiments that could get them closer to seeing results.
You can apply this process to any type of eating change, from trying out intermittent fasting to experimenting with an oil-free diet.
The best part? It puts your client in control of their experience and in a position to learn through action. And it casts you, the coach, as a source of strategy, guidance, and support—instead of a nutrition documentary fact-checker.
Remember: It’s all about your client.
Sensational documentaries can be challenging for coaches to deal with. Trust us, we get it.
But for many people, these docs are their first exposure to nutrition science. It makes sense your client would be convinced by, and maybe even concerned about, what they saw in a film.
Listen intently. Show empathy. Be their ally.
Using this framework, you can ease your client’s anxiety, harness their enthusiasm, and help create an effective plan that feels right to them.
And you can be 100 percent certain: Those are serious game changers.
If you’re a coach, or you want to be…
Learning how to coach clients, patients, friends, or family members through healthy eating and lifestyle changes—in a way that makes them feel empowered and motivated—is both an art and a science.
If you’d like to learn more about both, consider the Precision Nutrition Level 1 Certification. The next group kicks off shortly.
What’s it all about?
The Precision Nutrition Level 1 Certification is the world’s most respected nutrition education program. It gives you the knowledge, systems, and tools you need to really understand how food influences a person’s health and fitness. Plus the ability to turn that knowledge into a thriving coaching practice.
Developed over 15 years, and proven with over 100,000 clients and patients, the Level 1 curriculum stands alone as the authority on the science of nutrition and the art of coaching.
Whether you’re already mid-career, or just starting out, the Level 1 Certification is your springboard to a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results.
[Of course, if you’re already a student or graduate of the Level 1 Certification, check out our Level 2 Certification Master Class. It’s an exclusive, year-long mentorship designed for elite professionals looking to master the art of coaching and be part of the top 1% of health and fitness coaches in the world.]
Interested? Add your name to the presale list. You’ll save up to 30% and secure your spot 24 hours before everyone else.
We’ll be opening up spots in our next Precision Nutrition Level 1 Certification on Wednesday, April 8th, 2020.
If you want to find out more, we’ve set up the following presale list, which gives you two advantages.
- Pay less than everyone else. We like to reward people who are eager to boost their credentials and are ready to commit to getting the education they need. So we’re offering a discount of up to 30% off the general price when you sign up for the presale list.
- Sign up 24 hours before the general public and increase your chances of getting a spot. We only open the certification program twice per year. Due to high demand, spots in the program are limited and have historically sold out in a matter of hours. But when you sign up for the presale list, we’ll give you the opportunity to register a full 24 hours before anyone else.
If you’re ready for a deeper understanding of nutrition, the authority to coach it, and the ability to turn what you know into results… this is your chance to see what the world’s top professional nutrition coaching system can do for you.
The post How to talk to your clients (and mother) about the newest Netflix nutrition documentary appeared first on Precision Nutrition.
Source: Health1
As his weight climbed to nearly 300 pounds, Dominic Matteo thought he knew how to turn things around: Just stop eating chips, ice cream, and other highly processed foods.
“I’ll will myself through this,” he told himself.
Then he’d see the ice cream in the freezer and think, ‘Just one spoonful.’ Soon Matteo was staring at an empty container and wondering, ‘Why am I so weak?’
But Matteo’s willpower wasn’t the problem—his kitchen was. It was stocked with tempting junk foods, and it needed a serious overhaul.
Here’s the thing: Back then, Matteo didn’t believe a kitchen makeover would actually work. It sounded too easy.
He tried it anyway, though… and went on to lose over 100 pounds.
“If I hadn’t done that experiment, I probably wouldn’t have been successful,” says Matteo, who’s now a Precision Nutrition Level 2 Master Class coach. “It’s all about self-discovery and awareness.”
At Precision Nutrition, we often use experiments to help our clients discover important clues about what they really need (and don’t need) to reach their goals. Such experiments serve as powerful tools for uprooting the limiting and often false beliefs that tend to derail lasting habit change.
In this article, you’ll find three of our most transformative experiments. Try them yourself (or use with a client). What you learn may help you finally clear your biggest hurdles… even if the experiments sound too easy to work.
Limiting Belief #1: “If I had more willpower, I could stop eating so much junk food.”
Many of us assume, much like Matteo did, that willpower is something we’re either born with… or we’re not.
So when we find ourselves reaching for the second (or third … or fourth … or fifth) chocolate chip cookie, we beat ourselves up for being “weak.”
But portion control and healthful food choices are less about motivation and willpower and more about your environment. Give this experiment a try, and you’ll see what we mean.
The experiment: Do a kitchen makeover.
Use this two-step process to clean out your fridge, pantry, freezer, and other places you stash food. In the process, you’ll make some foods a lot harder to eat and other foods a lot easier to eat.
Step 1: Make a list
Determine your red, yellow, and green light foods.
But keep in mind: At Precision Nutrition, we don’t believe in universally good or bad foods. Everyone’s red, yellow, and green lists will be different.
Here’s how to identify yours:
Red light foods = “no go” foods. These are foods that present such a difficult challenge for you that they just aren’t worth the struggle. Red light foods may not work for you because:
- They don’t help you achieve your goals
- You always overeat them
- You’re allergic to them
- You can’t easily digest them
- You just don’t like them
Ultra-processed foods often fall into this category.
Yellow light foods = “slow down” foods. Maybe you can eat a little bit of these and stop, or you can eat them sanely at a restaurant with others, but not at home alone.
Green light foods = anytime foods. They’re nutritious and make your body and mind feel good. You can eat them normally, slowly, and in reasonable amounts. Whole foods usually make up most of this list.
Live with other people? Try these client-tested strategies.
So what if your partner or kids love the foods that you want to get out of the house?
Matteo confronted this exact predicament. Here’s what he suggests.
Talk about it. Explain that you want to make a change—and why. You might say, “I really need your help. I can’t do this alone.”
Take small steps. Focus on removing or reducing a couple of foods at a time rather than every single red light food at once.
Compromise. For example, rather than purchasing half-gallon containers of ice cream, Matteo’s family now buys eight single-serving cups—just enough for each family member to consume two single-serving desserts a week.
Stash it out of sight. If you must keep a red light food in the house, make it as difficult to access as you can. For example, you might keep chips on a shelf in the basement rather than in the kitchen. One of Matteo’s clients asked his wife to store desserts in a safe for which only she knew the combination.
Step 2: Get cleaning.
You’ll probably need a large garbage bag (maybe a few!) and a compost bin, if you have one.
First, get rid of the red light foods. If you struggle with the idea of wasting food, consider donating unopened, non-perishable, unexpired items to a charity. Compost what you can’t donate.
And remind yourself: Overeating is no less wasteful than trashing the food, given your body doesn’t actually need the calories. Plus, you just might find, as Matteo did, that your kitchen purge actually saves you money over time because you’ll stop buying certain foods.
Next, deal with the yellow light foods. You have a few options here. You can remove them, keep them in smaller quantities to prevent overeating, or put them somewhere hard to see and reach (on a high shelf in an opaque container, for example).
Lastly, stock up on your green light foods. Put these foods front and center and take steps to make them easy to grab and eat.
For example, maybe you make your own trail mix, storing it at the front of the pantry where you’re more likely to see it. Or, perhaps you peel a couple of oranges and keep them toward the front of the fridge, for easy snacking during your laziest moments. Or maybe you keep a half dozen hard-boiled eggs on the ready.
One note: Don’t overdo it when purchasing new green foods, especially produce, as they’re likely perishable (unlike most of the red and yellow foods you’re replacing). Remember, it’s okay to start small and build from there.
Step 3: Take notes.
The next time you get a craving for a red or yellow food, notice what happens. Do you reach for something on your green light list, since that’s what’s right in front of you? Or do you drive to the store to get food you crave? Or… do you decide not to eat anything at all because it requires way too much effort?
The lesson: Your environment makes it harder to practice healthy eating habits.
“Understanding that your environment guides your decisions can facilitate better actions,” Matteo says.
What he’s getting at is something we refer to as Berardi’s First Law (named after our co-founder, John Berardi, PhD):
If a food is in your house or possession, either you, someone you love, or someone you marginally tolerate, will eventually eat it.
There’s also a corollary to this law:
If a healthy food is in your house or possession, either you, someone you love, or someone you marginally tolerate, will eventually eat it.
This is why relying on willpower or motivation is a fundamentally flawed plan. No matter how much or how little willpower you actually have, you’ll eventually default to the easiest food options, especially when you’re tired. Or stressed. Or ravenous.
By removing red light foods, you make the choice to eat green foods so much easier—almost no willpower required.
Limiting Belief #2: “I hardly eat anything, and I still can’t lose weight.”
Feeling this way can be incredibly frustrating and confusing. Sometimes, it even stops people from trying to get healthier altogether.
But in every case, the principle of energy balance applies:
When you eat more calories (energy) than you expend, you gain weight. And when you eat fewer calories than you expend, you lose weight. (Which sounds way simpler than it is, of course.)
So what gives? Let’s find out.
The experiment: For one week, track everything you eat.
All you have to do: Write down what you eat every day for a week.
Yeah, yeah, yeah. You’ve heard this advice before—maybe hundreds of times.
But have you really done it? By actually writing it down (versus keeping a mental tally)?
For every single meal and snack?
Every day?
For a whole week?
If not, give it a try. It’s actually a lot easier than it sounds. You can write it down in a notebook, use a record-keeping app like MyFitnessPal, or even just snap a photo of everything you eat.
Make sure to include everything you eat and drink. Don’t forget to record the cream and sugar in your coffee, the dressing on your salad, and the lone fry (or was it eight?) you stole off your kid’s plate.
(Note: Unless you enjoy it, we’re not recommending you track this way regularly. This is just a short-term experiment.)
Treat these notes as if you were a scientist. This isn’t about judging your food choices. It’s merely about noticing them. Be kind, curious, and compassionate with yourself.
For the most accurate snapshot of your eating habits, try to do this during a typical week without any big events, and don’t change how you normally eat just because you’re keeping track.
At the end of the week, take a look at your log. Is it in line with how much you thought you were eating?
The lesson: It’s easy, and incredibly common, to underestimate how much you eat.
Research shows that, on average, people underestimate their food intake by around 47 percent—for all sorts of understandable reasons.
First, mindless nibbles can be even less memorable than the storage location of our car keys.
Second, though humans are great at a lot of things, estimating portion sizes just isn’t one of them. We don’t always recognize how caloric certain foods are (hi, peanut butter), and sometimes we deceive ourselves. (‘I had, like, five chips… not three-quarters of the bag… right?”)
Point is, this is a real thing. And it happens to a lot of people—even dietitians.
That’s why many people need nutritional guard rails—calorie counts, macros, or hand portions—to guide what and how much they eat… at least for a little while. Here at PN, we use hand portions to help clients make better food and portion judgments. (We’ve seen some incredible transformations using this method alone.)
If you haven’t already checked out our Nutrition Calculator, go ahead and plug in your goals and personal info. You’ll get a full report of how much to eat, along with the corresponding hand portions, and everything you need to know about how they work.
Using this approach, in combination with mindful eating practices like eating slowly and to 80 percent full, can help you eat in a way that makes weight loss feel more effortless.
3 more experiments to try
Want to keep learning more about yourself? Try the following to keep gathering intel.
Experiment: Eat nothing but sugar packets (read: pure sugar) for a day. (Good luck!)
What it shows: Sugar itself may not really be a problem food for you. Read: Most people won’t stuff themselves with sugar alone. Instead, it’s more about what the sugar is mixed with. For example, you may be okay consuming it when it’s in fruit, yogurt, or even ketchup, but not when it’s inside your personal red light foods like cookies, chocolate, or ice cream.
Experiment: Eat slowly every day for a month, trying to make every meal last a little bit longer. (Start by taking a breath between bites.)
What it shows: You may discover that you feel more satisfied sooner, so you eat less automatically. You may also notice eating slowly brings up uncomfortable feelings—ones you’ve been quashing with food.
Experiment: Use this article to make breakfast a little bit healthier.
What it shows: You don’t have to do a complete 180 in order to see progress. Could you swap cold cereal for oatmeal? Could you have fruit instead of hashbrowns? Could you try eggs on a bed of greens instead of with a bagel? It’s not just about the substitutions; it’s about being thoughtful about what you eat… before you eat. Small changes, done consistently, pave the way to lasting habits.
Limiting Belief #3: “I seriously can’t handle being hungry.”
Hunger is a lot of things: annoying, uncomfortable, distracting…
One thing it’s not: such a big deal that you should do everything in your power to avoid ever experiencing it.
Problem is, hunger feels like a big deal. Some clients have even told us that hunger feels like an emergency. They worry that if they don’t eat right away, their hunger will continue to get worse and worse and worse until… they die.
Or wish they could.
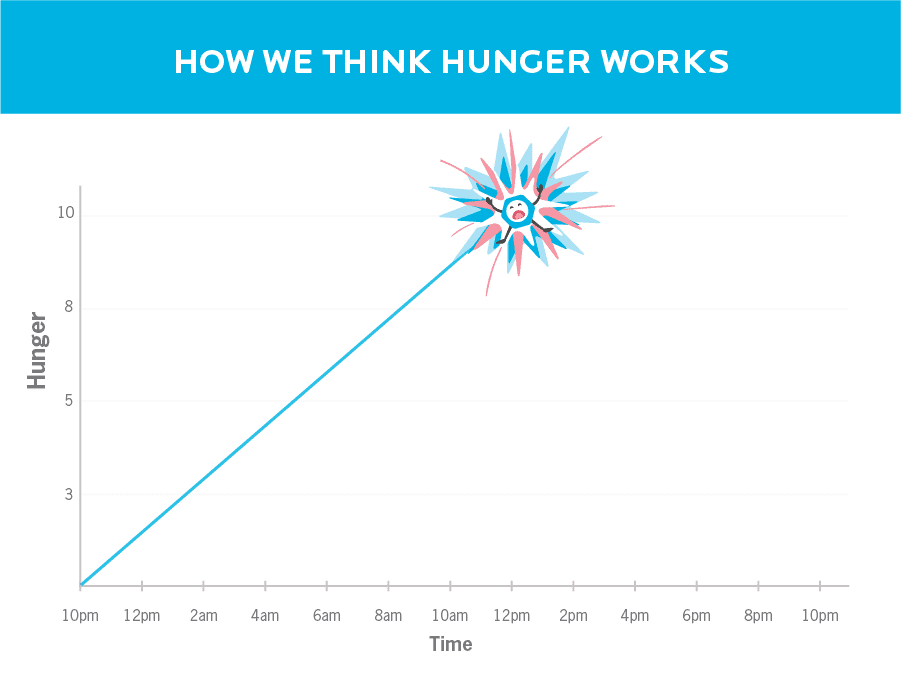
For these reasons, many people eat as soon as they feel even the slightest pang—physical or mental. That often means they consume more than really needed, which leads to weight gain (or stalls fat loss). They also reach for whatever they find first (see experiment #1).
But what happens when you don’t immediately meet hunger with food? Let’s find out.
The experiment: Try fasting for a day.
We know it sounds scary. Nothing bad will happen—promise.
We include this experiment, lovingly called “fasting day,” in our year-long coaching program. Over the years, our coaching clients have told us this day is one of the most impactful experiences of the entire program.
Here’s how it works: Consume no calories for 24 hours.
Zero. Nada. None.
Enjoy calorie-free drinks such as water, flavored water, unsweetened tea, or plain coffee. But other than that, avoid all food and caloric beverages.
Obviously this isn’t something we recommend long-term. It’s just one day.
And it just might be the most challenging and insightful day you’ve had in a long time.
A couple of important caveats:
You can do this on a schedule that works for you. For example, you could fast from dinner to dinner, or lunch to lunch. If 24 hours feels like too much, consider just skipping a meal or two instead. This isn’t about getting it “perfect.” Also, it might go without saying, but you probably shouldn’t try this experiment on a day when you need to be 100% “on your game,” such as when you’re flying a plane or doing open-heart surgery.
Fasting isn’t right for everyone. Do not fast if you:
- have a medical condition that requires you to eat
- struggle with disordered eating and have been told never to fast
- know that periods of food restriction—even if done carefully and consciously—can lead to bingeing later on
The lesson: Hunger isn’t an emergency.
It’s natural to worry that hunger will keep getting worse and worse—making us feel lousy and preventing us from getting anything useful done.
But hunger doesn’t work like that.
Hunger hormones are released in waves based on when our bodies are expecting food.
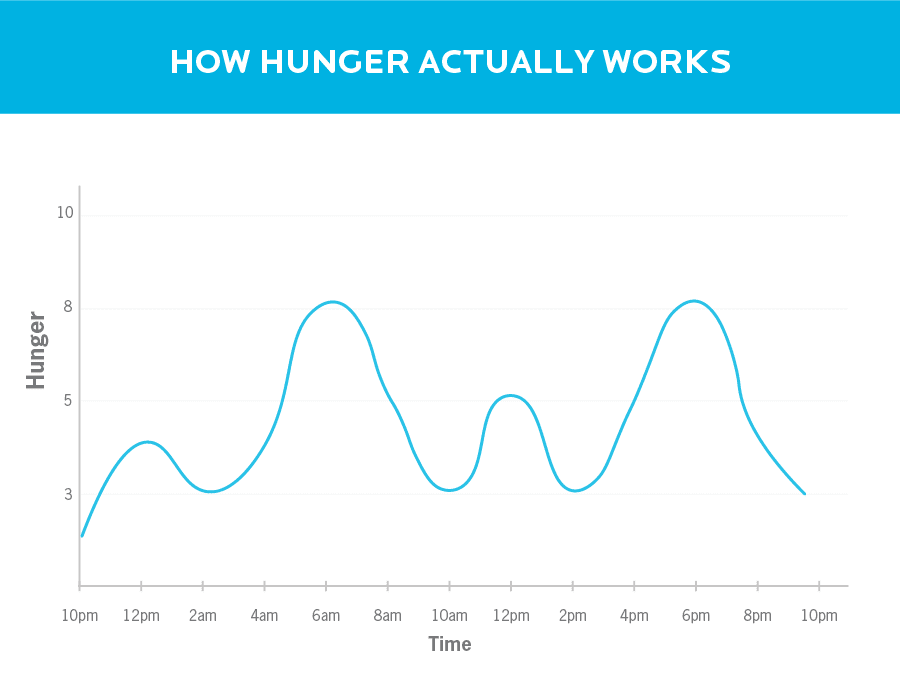
As you’ll probably experience while doing this experiment, hunger is strongest around the three- to four-hour mark of a fast. Then it subsides.
It’s an incredible feeling (and often a great relief) to learn that you can feel hungry—truly hungry—and choose not to do anything about it.
There are several benefits here:
- Benefit #1: If the available food choices don’t make sense for you, you know you can wait until something better is available. No biggie.
- Benefit #2: You learn what true hunger feels like. This awareness can help you distinguish psychological hunger (“I feel like eating something”) from physiological hunger (“My body is telling me it’s time to eat”).
- Benefit #3: If it’s not “time to eat,” waiting until your next meal or snack won’t feel like a problem. This is not only convenient if hunger strikes somewhere food isn’t accessible (such as on your commute), but can also be extremely helpful if you’re trying to lose fat.
Keep experimenting, keep growing.
You can probably see why we’re such big fans of self-experimentation: It’s quite literally a win-win. You’ll either get a reaffirming boost of confidence and confirmation that you’re already on the right track, or you’ll get valuable information about how you can change things for the better.
By simply paying attention to how experiments make you feel, you empower and energize yourself to make better, more informed choices.
And remember: Self-experimentation isn’t about getting it perfect. It’s about finding out what works for you, and then putting it into practice—one small step at a time.
Want help becoming the healthiest, fittest, strongest version of you?
Most people know that regular movement, eating well, sleep, and stress management are important for looking and feeling better. Yet they need help applying that knowledge in the context of their busy, sometimes stressful lives.
Over the past 15 years, we’ve used the Precision Nutrition Coaching method to help over 100,000 clients lose fat, get stronger, and improve their health… for the long-term… no matter what challenges they’re dealing with.
It’s also why we work with health, fitness, and wellness professionals (through our Level 1 and Level 2 Certification programs) to teach them how to coach their own clients through the same challenges.
Interested in Precision Nutrition Coaching? Join the presale list; you’ll save up to 54% and secure a spot 24 hours early.
We’ll be opening up spots in our next Precision Nutrition Coaching on Wednesday, January 15th, 2020.
If you’re interested in coaching and want to find out more, I’d encourage you to join our presale list below. Being on the list gives you two special advantages.
- You’ll pay less than everyone else. At Precision Nutrition we like to reward the most interested and motivated people because they always make the best clients. Join the presale list and you’ll save up to 54% off the general public price, which is the lowest price we’ve ever offered.
- You’re more likely to get a spot. To give clients the personal care and attention they deserve, we only open up the program twice a year. Last time we opened registration, we sold out within minutes. By joining the presale list you’ll get the opportunity to register 24 hours before everyone else, increasing your chances of getting in.
If you’re ready to change your body, and your life, with help from the world’s best coaches, this is your chance.
[Note: If your health and fitness are already sorted out, but you’re interested in helping others, check out our Precision Nutrition Level 1 Certification program].
The post 3 diet experiments that can change your eating habits—and transform your body (even if they seem way too easy to work). appeared first on Precision Nutrition.
Source: Health1
Bernie and Paul spent the past 12 months transforming their eating habits, health, bodies, and lives with personal help from a PN coach. And now? They’re our latest Grand Prize winners. See how we surprised them with $25,000 each, and meet the rest of our January 2020 Precision Nutrition Coaching winners.
++++
Every six months, in our Precision Nutrition Coaching program, we give away more than $125,000 to the men and women who have the most incredible, inspiring body transformations.
Yep, that’s more than $250,000 a year.
And today, you’ll meet our latest amazing winners.
These folks started working with us in January 2019 and—over the course of the past year—completely transformed how they eat, move, look, and feel.
They lost weight, gained strength, boosted their health, and inspired their friends and families.
What’s more, they did all of this without extreme diets or crazy workout routines. There were no meal plans or off-limit foods. No unbreakable rules. No deprivation. And perhaps best of all, no guilt.
Each person simply committed to making a change, stayed consistent, and used the accountability and support of one of our dedicated coaches.
- Meet Bernie, our Women’s $25,000 Grand Prize Winner
- Meet Paul, our Men’s $25,000 Grand Prize Winner
- See photos of all January 2020 Women’s winners
- See photos of all January 2020 Men’s winners
$25,000 Grand Prize Winner: Bernie

Lost 45 lbs and 42 total inches!
Age: 46 years
Weight Lost: 45 lbs (from 165 lbs to 120 lbs)
Total Inches Lost: 42 inches (from 228 inches to 186 inches)
Weight Lost: 45 lbs (from 165 lbs to 120 lbs)
Total Inches Lost: 42 inches (from 228 inches to 186 inches)
Bernie Stewart just couldn’t bear to show her arms.
That pretty, strappy top she’d so optimistically bought during a fit phase?
She felt she had to cover it up with a bolero cardigan.
She was also wearing what she calls her “Ali Baba” pants—voluminous and drapey enough to disguise the lumps and bumps underneath.
Hunched over a coffee, she stared at her tablet, desperately looking for something, anything to take her away from the endless round of diets.
After 35 years of fluctuating weight, 35 years of binge eating and emotional eating, 35 years of feeling guilty and ashamed, Bernie was fed up.
Now 46 years old and with two young children watching her every move, Bernie knew this wasn’t just about her any more.
Sure, she wanted to look great. She wanted to feel fit and healthy. But more than that, she wanted to set a positive example.
She wanted to change her attitudes to food and to herself. Precision Nutrition Coaching showed her how.
“My issues with food and self-hatred were shocking.”
“At the start, I was still working with old conditioning,” Bernie says. She was the kind of person who could eat an entire pizza with a large side of chips, follow up with some cheesecake, and wash it all down with pints of sherry.
She liked the feeling of fullness, the way that rich and fatty food could numb her. Overeating was a pleasure and a comfort.
But it was also a kind of curse, dooming her to a constant and nasty internal chorus. “I was self-berating, guilt-ridden, self-flagellating,” she says.
Bernie knew she needed help to make a lasting change. From the moment she signed up for coaching, Bernie gave it her best.
Every time she clicked on a new day’s lesson or habit, she considered it a gift, and her passion and focus never wavered. By staying consistent and trusting the process, she lost some weight in the first month.
But the next few months tested her patience. The scale seemed to plateau and improvements weren’t as visible. Yet Bernie stayed the course.
In retrospect, Bernie sees she wasn’t really stagnating—she was laying the groundwork for deeper change.
Precision Nutrition didn’t promise a quick fix, like diets she’d tried in the past. Instead, it gave her the tools for a total transformation.
Among those tools was self-forgiveness.
For the first time in her adult life, Bernie didn’t interpret mistakes as signs of failure. Instead, she saw them as steps in a learning process.
“With this one change, I felt like a new person,” Bernie says.
She stopped blaming herself. Her guilt began to fade. A metaphorical weight had lifted, and with it, the physical weight began to melt away.
She started to feel more energetic. She had more fun with her kids. They noticed she was happier. Her friends noticed she was happier.
“I was more confident, clothes were fitting better, I was starting to see muscles, I was gaining strength.”
What surprised her most was how easy it all felt.
“Just one small step at a time, no pressure and no strain or stress!” Bernie says.
Watch the video below to see Bernie’s priceless reaction to winning our $25,000 grand prize.
Want to get results like Bernie? Learn more about the Precision Nutrition Coaching Program for Women.
$25,000 Grand Prize Winner: Paul

Lost 22 lbs and 13 total inches!
Age: 37 years
Weight Lost: 22 lbs (from 172 lbs to 150 lbs)
Total Inches Lost: 13 inches (from 230 inches to 217 inches)
Weight Lost: 22 lbs (from 172 lbs to 150 lbs)
Total Inches Lost: 13 inches (from 230 inches to 217 inches)
There was a time in his life when Paul LeTourneau found it difficult to gain weight.
Eventually, he got so frustrated that, in order to beef up, he joined Scrawny to Brawny, a predecessor to Precision Nutrition Coaching.
It worked, too. Paul gained 22 pounds, became a finalist in that program, and was happier with his body and his fitness than he’d ever been.
But just as the program ended, Paul hurt his back. He had to go easier on his workouts. And then, over time, life got complicated. Work, more work, family stuff—the usual. Meanwhile, his metabolism was starting to slow down.
Bit by bit, his body composition was morphing from muscle to fat—almost without his knowledge.
Paul was eating the way you have to eat when you’re a skinny guy who wants to bulk up.
But he wasn’t that skinny guy any more.
Now, he was famous among his friends for gorging himself at buffets–those all-you-can-eat smorgasbords seemed made for him.
Meals always involved seconds. Sometimes even thirds. And when it came to snacks, he could swallow a large bag of chips without blinking.
At 37, Paul looked in the mirror and saw a belly for the first time in his life.
He was also waking up with throbbing headaches. He knew he had to make a change, so he signed up for Precision Nutrition Coaching.
By the end of his first month in nutrition coaching, Paul was seeing improvements. He loved the way the program helped him track and measure his progress.
He started getting compliments from people at work. The morning headaches soon disappeared.
Then he injured his neck at the gym. The problem wasn’t serious, but it meant he had to cut back on his workouts for a while.
“In the past when I hit a roadblock, I’d probably give up. I’d figure, if I can’t go full out, why bother?”
This time, with his coach, Craig Weller’s help, he found ways to adapt his workouts and stay active. Instead of indulging in “all or nothing” thinking, Paul kept his goal in mind and looked for what he could do.
And with that one small change, he inaugurated a whole new mindset.
Paul’s goal, from the start, was to improve his relationship with food. But this meant a shift in his identity.
For years, overeating had been a kind of gimmick for him. It was the quality that friends knew him for, and one they seemed enjoyed him about him. Fifty-two wings in a sitting. Fifty chicken nuggets. It became a game to keep track of it all.
So, when he started to eat slowly and have smaller portions, he faced some ribbing and pushback from the crowd.
Where did the old Paul go? Who was this new version? Maybe he wouldn’t have as much fun. Maybe he wouldn’t be as much fun.
Maybe he wouldn’t be as manly.
Those were the thoughts that percolated in his mind (and his friends’ minds) as he started to change his behaviors.
It took determination and courage to stay true to his goals.
Especially when the little voice in his head was telling him that losing weight would also mean losing muscle mass.
“Heavier can seem better for a guy,” he explains. When “big” and “strong” always go together, it doesn’t feel good when the scale starts to drop—even when you know you need to lose some fat.
But with his coach’s guidance, Paul began to understand that in trying to maintain a very high weight along with visible muscle, he was actually ignoring his natural body type and doing himself a disservice.
“My bones are small. My frame isn’t made to carry a lot of weight.”
Now, instead of aiming to be heavy and strong, Paul aims to be the strongest he can be—at the lightest he can be.
It’s a question of emphasis and balance.
Today, Paul is focused on reaching his own personal best—not someone else’s.
These days, he may not be packing in as many wings at the buffet table, but he’s enjoying his food a whole lot more.
And at 22 pounds leaner, he’s also stronger and fitter than he’s ever been.
“Everyone can be successful in this program,” Paul says.
“It’s like that proverb about the difference between giving a man a fish and teaching a man to fish,” he adds. “This program gives you the tools to stay fit and healthy for life.”
Watch the video to see Paul’s awesome reaction to hearing he won our $25,000 grand prize.
Want to get results like Paul? Learn more about the Precision Nutrition Coaching Program for Men.
Meet our other Women’s winners

Elizabeth
$10,000 Women’s Winner
Age: 53 years
Weight Lost: 44 lbs (158 lbs to 114 lbs)
Total inches lost: 37″ (220″ to 183″)
PN taught me the power of small, consistent efforts. This approach enabled me to achieve greater physical transformation than I dreamed possible—step by step. It also helped me recognize how I’d been limiting myself, and encouraged me to imagine the person I wanted to become.
– Elizabeth

Claire
$10,000 Women’s Winner
Age: 25 years
Weight Lost: 32 lbs (199 lbs to 167 lbs)
Total inches lost: 24″ (236″ to 212″)
I joined PN Coaching because I wanted to eat healthy, move more, and stay that way for life. This year I’ve accomplished those goals and much more. I’ve learned to prioritize my physical and mental health, which has given me more energy and confidence in my daily life than I ever thought possible!
– Claire

Alison
$2,500 Women’s Winner
Age: 65 years
Weight Lost: 20 lbs (147 lbs to 127 lbs)
Total inches lost: 18″ (204″ to 186″)
Precision Nutrition’s unique coaching program transformed me from a burnt-out, unmotivated, wannabe competitor into an energized, engaged, lean, never-quit athlete. I cannot speak highly enough of the evidenced-based content, superb coaching staff, and vibrant online community.
– Alison

Sarah
$2,500 Women’s Winner
Age: 59 years
Weight Lost: 27 lbs (187 lbs to 160 lbs)
Total inches lost: 25″ (216″ to 191″)
I’m happy with the changes I’ve made physically and mentally. Most importantly, it was the lessons learned and the process of taking care of myself that made my journey a success. Am I perfect? No. Am I happy with not being perfect? Yes. Is the journey done? Never!
– Sarah

Lacey
$2,500 Women’s Winner
Age: 37 years
Weight Lost: 34 lbs (159 lbs to 125 lbs)
Total inches lost: 29″ (229″ to 200″)
PN is not a race, it is a journey. It has taught me how to relax, enjoy, and accept myself. If you let go and trust the program, big changes and great things will happen.
– Lacey

Lindsay
$2,500 Women’s Winner
Age: 40 years
Weight Lost: 27 lbs (173 lbs to 146 lbs)
Total inches lost: 11″ (221″ to 210″)
When I started viewing adjustments to my exercise routine and habits as experiments, I finally got in tune with my body and started seeing changes. I now consider a cohesive view of my health, including sleep, my support system, and managing stress—not just calories and cardio.
– Lindsay

Melinda
$1,000 Women’s Winner
Age: 37 years
Weight Lost: 24 lbs (145 lbs to 121 lbs)
Total inches lost: 21″ (204″ to 183″)
PN Coaching is the perfect blend of accountability, encouragement, and education. My balance and strength has improved, not just physically, but mentally and emotionally too.
– Melinda

Faith
$1,000 Women’s Winner
Age: 39 years
Weight Lost: 21 lbs (154 lbs to 133 lbs)
Total inches lost: 20″ (219″ to 199″)
My main goal this past year with Precision Nutrition was to be more consistent. By planning and making better choices month after month, I slowly started seeing results. I’m working on ditching my all-or-nothing mindset and have made fitness a part of my life instead of being on a strict diet and doing super high intensity workouts for a short period of time. Now, I show up day after day because it’s just who I am!
– Faith

Laurel
$1,000 Women’s Winner
Age: 55 years
Weight Lost: 18 lbs (154 lbs to 136 lbs)
Total inches lost: 20″ (222″ to 202″)
Overworked, overtired, overweight, and over-care-taking; the idea of a coach in my corner sounded wonderful. I decided to follow PN’s program as sincerely as I could each day. The daily habits and lessons steered me gently through many challenges to a much more resilient, playful, and higher quality of life. A newfound sense of ease was the biggest surprise. Priceless.
– Laurel

Katherine
$1,000 Women’s Winner
Age: 38 years
Weight Lost: 27 lbs (175 lbs to 148 lbs)
Total inches lost: 30″ (224″ to 194″)
The Precision Nutrition program and team supported me and challenged me to become the best version of myself. Over the course of a year, I changed the way I approach eating and exercise. And probably for the first time ever, I can embrace and celebrate the limitless possibilities of what it means to be me.
– Katherine

Jen
$1,000 Women’s Winner
Age: 57 years
Weight Lost: 40 lbs (227 lbs to 187 lbs)
Total inches lost: 36″ (267″ to 231″)
My year with PN is reflected in the opening line of one my favorite poems: ‘Finally on my way to yes, I bump(ed) into all the places where I said no to my life’. In those moments, PN was there to help if I needed it, and YES is an amazing place to be.
– Jen

Cherie
$1,000 Women’s Winner
Age: 59 years
Weight Lost: 12 lbs (126 lbs to 114 lbs)
Total inches lost: 14″ (207″ to 193″)
Before PN, I worked very hard at exercising and cooking healthy foods, but my appearance didn’t reflect my efforts and intentions. I felt frumpy and matronly. Now, as I complete my PN journey, I feel like my appearance reflects my values of fitness, strength, healthy eating, and hope for the future!
– Cherie

Alexandra
$1,000 Women’s Winner
Age: 47 years
Weight Lost: 15 lbs (141 lbs to 126 lbs)
Total inches lost: 16″ (216″ to 200″)
This has been a year of major, unanticipated changes for me in all areas of my life. PN was not only the consistent rudder throughout the year, but also a source of friendly prods, thoughtful workshops, ideas to consider, and important accountability. I am stronger and leaner mentally and physically, and excited about what lies ahead.
– Alexandra

Julie
$1,000 Women’s Winner
Age: 38 years
Weight Lost: 20 lbs (190 lbs to 170 lbs)
Total inches lost: 40″ (244″ to 204″)
This is not just a lifestyle. It’s a discipline, and most importantly, a journey.
– Julie
Meet our other Men’s winners

Jacob
$10,000 Men’s Winner
Age: 40 years
Weight Lost: 120 lbs (359 lbs to 239 lbs)
Total inches lost: 77″ (331″ to 254″)
In many ways, I feel like I’m a totally different person now. PN helped me be accountable to myself and shift my mindset about eating, exercising, and life in general. By working on one habit at a time, I have been able to make sustainable life changes. The lessons were always really relevant and applicable to my life.
– Jacob

Nick
$10,000 Men’s Winner
Age: 33 years
Weight Lost: 18 lbs (153 lbs to 135 lbs)
Total inches lost: 11″ (206″ to 195″)
It’s been an incredible year with PN. At the end of it I’m literally in the best shape of my life. I’ve eaten pretty well and worked out since high school, but it’s only been since learning to be consistent that I look and feel like an athlete. Just as awesome though have been the inner changes: I’m better privileging my own needs and letting go of chasing ‘perfect.’
– Nick

Paul
$2,500 Men’s Winner
Age: 57 years
Weight Lost: 33 lbs (229 lbs to 196 lbs)
Total inches lost: 23″ (257″ to 234″)
A lean lifestyle? I never knew such a thing existed. With PN by my side, I’m now planning on dying young at heart at a ripe old age!
– Paul

Daniel
$2,500 Men’s Winner
Age: 36 years
Weight Lost: 46 lbs (209 lbs to 163 lbs)
Total inches lost: 37″ (246″ to 209″)
This year has been amazing! PN has changed the way I look at life and its challenges. They are no longer difficult or impossible. Now, they’re easier to grasp, take charge of, and accomplish.
– Daniel

John
$2,500 Men’s Winner
Age: 39 years
Weight Lost: 47 lbs (263 lbs to 216 lbs)
Total inches lost: 28″ (265″ to 237″)
Come for the fitness, stay for the life lessons. PN taught me how to recognize my underlying fitness goals (beyond the superficial ones) and how to balance those goals against the rest of the commitments in my life with fundamental, long-term strategies.
– John

Ted
$2,500 Men’s Winner
Age: 69 years
Weight Lost: 22 lbs (200 lbs to 178 lbs)
Total inches lost: 10″ (233″ to 223″)
The PN program has given me the opportunity to improve my fitness to a level I could have only dreamed of before. It also gave me eating habits that are realistic and not impossible to follow. If you follow the program, you will see results.
– Ted

Venkatraghavan
$1,000 Men’s Winner
Age: 42 years
Weight Lost: 24 lbs (160 lbs to 136 lbs)
Total inches lost: 15″ (220″ to 205″)
This year I learned it’s almost always never about the food. I’ve shaped my life to be more focused, dealt with deep-rooted patterns that were holding me back, and built deep self-awareness. The care, kindness, and compassion I received from the PN team translated into me in allowing myself these courtesies. I’m now committed to supporting others as they learn about and shape their lives through food.
– Venkatraghavan

Jeff
$1,000 Men’s Winner
Age: 49 years
Weight Lost: 25 lbs (228 lbs to 203 lbs)
Total inches lost: 14″ (246″ to 232″)
Along with losing weight and achieving a level of fitness that I’ve never obtained before came an unexpected byproduct: mental strength. I’ve replaced anxiety and self-consciousness with a calmer more relaxed mindset and confidence. Not constantly thinking about my weight, what I look like, or expecting perfection of myself feels like freedom from my old self. Thank you PN!
– Jeff

RJ
$1,000 Men’s Winner
Age: 40 years
Weight Lost: 41 lbs (319 lbs to 278 lbs)
Total inches lost: 35″ (298″ to 263″)
As a small business owner, I’ve had a crazy-stressful year. But with the help and constant support of PN Coaching, I was able to better understand and overcome obstacles that would have knocked me off track in the past.
– RJ

Nick
$1,000 Men’s Winner
Age: 41 years
Weight Lost: 31 lbs (190 lbs to 159 lbs)
Total inches lost: 22″ (242″ to 220″)
One of the biggest things I got from my PN journey is that consistency really does beat perfection. There were loads of times that I had to scale back the workouts or eat less-than-perfect meals, but I always tried to make positive choices given the options or time available. My coach helped me to see those instances as successes—more so, actually, than when everything felt easy.
– Nick

Michael
$1,000 Men’s Winner
Age: 38 years
Weight Lost: 44 lbs (253 lbs to 209 lbs)
Total inches lost: 23″ (269″ to 246″)
Precision Nutrition told me to slow down, breathe, and just focus on the next rep, set, bite, or meal. And to let go of the past, welcome each new day, and celebrate every victory, no matter how small. It doesn’t sound like a lot, but this has helped me reclaim my life and be who I want to be.
– Michael

Craig
$1,000 Men’s Winner
Age: 42 years
Weight Lost: 48 lbs (242 lbs to 194 lbs)
Total inches lost: 36″ (268″ to 232″)
The biggest impact the program had was developing my self-esteem and confidence. I’d always talked myself out of long-term physical fitness, but I realized I shouldn’t give up on anything until I give it a shot. A lot of the lessons helped change my mindset, not just about fitness, but in life. Questioning negative thought patterns and being mindful in all parts of my life have paid HUGE dividends for me. I also learned that you don’t need a perfect plan to start something. Always take action instead of waiting for the ‘right time’ to do something.
– Craig

Michael
$1,000 Men’s Winner
Age: years
Weight Lost: 57 lbs (362 lbs to 305 lbs)
Total inches lost: 20″ (306″ to 286″)
PN has provided me with the ability to free myself from fear of hunger, anxiety about hitting a specific workout schedule, and an all-or-nothing attitude. My progress actually accelerated when I slowed down, which forced me to focus on and enjoy the process.
– Michael

Jonny
$1,000 Men’s Winner:
Age: 25 years
Weight Gained: 10 lbs (from 187 lbs to 197 lbs)
Total inches gained: 11″ (224″ to 235″)
My year-long experience with PN has taught me the methodology and discipline it requires in order to naturally build muscle. PN provided me with excellent tools, wonderful educational materials, and support as needed in my efforts to achieve this end. The setup of the system, complete with the online platform, enables anyone who is willing to put in the work to succeed.
– Jonny
Meet a few hundred more Precision Nutrition clients.
To view all the men’s and women’s finalists from the January 2020 Coaching Program, click the links below.
- January 2020 Precision Nutrition Coaching for WOMEN finalists
- January 2020 Precision Nutrition Coaching for MEN finalists
To view all the men’s and women’s finalists from all of our Precision Nutrition Coaching programs, click one of the links below.
- Precision Nutrition WOMEN’S Coaching: The Finalist Hall of Fame
- Precision Nutrition MEN’S Coaching: The Finalist Hall of Fame
Of course, if you’re interested in working toward a body or health transformation of your own, consider joining our next Precision Nutrition Coaching group. We’re opening up a few spots in the coming weeks.
Want to transform your body and health?
As you probably know, you won’t overhaul your body this dramatically by just logging time on a treadmill or reading health tips on Twitter.
Awesome, lasting, wow-what-happened-to-you transformations usually require personal attention from an expert coach.
And here’s the good news: Precision Nutrition Coaching will be accepting new clients very soon, at our lowest, most accessible price ever.
If you’re interested and want to find out more, I’d encourage you to join our presale list.
Being on the presale list gives you two special advantages.
- You’ll pay less than everyone else. At Precision Nutrition we like to reward the most interested and motivated people because they always make the best clients. Join the presale list and you’ll save up to 54% off the general public price, which is the lowest price we’ve ever offered.
- You’re more likely to get a spot. To give clients the personal care and attention they deserve, we only open up the program twice a year. Last time we opened registration, we sold out within minutes. By joining the presale list you’ll get the opportunity to register 24 hours before everyone else, increasing your chances of getting in.
[Note: If your health and fitness are already sorted out, but you’re interested in helping others, check out our Precision Nutrition Level 1 Certification program].
If you’re ready to change your body, and your life, with help from the world’s best coaches, this is your chance.
The post Precision Nutrition Coaching Grand Prize Winners: January 2020. We just surprised our latest winners with more than $125,000 in prizes! appeared first on Precision Nutrition.
Source: Health1
Just one year ago, these 20 men were inspired to make a change. To eat healthier, move better, and get stronger. Now, after 12 months of Precision Nutrition Coaching, that’s exactly what they’ve done. Transforming their health, bodies, and lives more than they ever thought possible.
They’ve realized that when it comes to living the life you want, your body can either be your greatest ally—or your fiercest enemy. And now, with the fit, capable body they’ve always wanted, they’re finally living life to the fullest. Boldly taking on each day with strength, health, and confidence.
They also have the chance to take home part of the $125,000 in prize money we’ve once again committed to this latest round of top clients. Scroll through these amazing photos and vote for the finalist whose transformation impresses you most.
++
Every year in Precision Nutrition Coaching, we help men and women from around the world dramatically improve their eating habits, exercise routine, and lifestyle.
With a world-class coach guiding and supporting them every step of the way, they lose weight, gain strength, and completely transform their bodies, health, fitness, and lives.
We also give clients a big, motivating goal to shoot for: $250,000 in cash prizes.
Consider it an antidote to the “you must suffer and feel guilty to get in shape” message you typically get from the fitness industry.
See, guys come to us wanting big changes:
- They want to lose weight, build muscle, and shed body fat.
- They want to feel physically and mentally strong.
- They want to make healthier food choices, consistently.
- They want to stop worrying about their health.
- They want to start doing all the awesome things they previously wanted to do but thought they couldn’t.
Above all, they want to become the fittest, strongest, healthiest versions of themselves.
In our experience, big, inspiring, life-changing goals like these are a whole lot easier to achieve when there’s a huge bonus at stake.
So, every six months, we divvy up a big pot of prize money for the best transformations among our male and female clients.
For the current group—which started in January 2019 and is wrapping up now—we’ve committed $125,000.
And right now, we need your help to choose our Men’s Grand Prize winner.
Help choose our Men’s Grand Prize winner (Top prize = $25,000)
The guys below started their Precision Nutrition Coaching journey in all shapes and sizes, and they hail from all parts of the globe. They knew building a leaner, stronger, healthier, body could make every part of their lives better. And they were tired of being “that guy”…
The one who keeps a t-shirt on at the pool or the beach. The one who’s fearful of what might show up in routine blood work at their next yearly check-up. The one too winded to enjoy playing soccer or chase with their kids (or grandkids).
They’re a diverse group with one thing in common: Now, after just 12 months of Precision Nutrition Coaching, they have the bodies and health they’ve wanted for a long time, and they’re confident they’ll stay this way for good.
How’d they do it?
No crash diets. No Biggest Loser-type bootcamps. And no full-time chefs.
Just research-based nutrition and lifestyle habits practiced daily—and personalized help from our expert coaches.
To vote for the guy you think should win the $25,000 Grand Prize, scroll through the photos below. Make your choice by clicking the “Vote for Finalist” button under the one you think achieved the best transformation.
But please don’t stop there. Once you’ve seen all the finalists and selected your #1 choice, scroll down to the bottom of this post.
At the bottom you’ll need to verify your choice. To do this, click the “Place your vote” button. This will log your vote and help us make our decision.
Thanks for your help!
Finalist #1
Lost 18 lbs and 11 total inches!
Age: 33 years
Weight Lost: 18 lbs (from 153 lbs to 135 lbs)
Total Inches Lost: 11 inches (from 206 inches to 195 inches)
Weight Lost: 18 lbs (from 153 lbs to 135 lbs)
Total Inches Lost: 11 inches (from 206 inches to 195 inches)
 Finalist #1 selected!
Finalist #1 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #2
Lost 33 lbs and 23 total inches!
Age: 57 years
Weight Lost: 33 lbs (from 229 lbs to 196 lbs)
Total Inches Lost: 23 inches (from 257 inches to 234 inches)
Weight Lost: 33 lbs (from 229 lbs to 196 lbs)
Total Inches Lost: 23 inches (from 257 inches to 234 inches)
Finalist #2 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #3
Lost 24 lbs and 15 total inches!
Age: 42 years
Weight Lost: 24 lbs (from 160 lbs to 136 lbs)
Total Inches Lost: 15 inches (from 220 inches to 205 inches)
Weight Lost: 24 lbs (from 160 lbs to 136 lbs)
Total Inches Lost: 15 inches (from 220 inches to 205 inches)
Finalist #3 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #4
Lost 31 lbs and 22 total inches!
Age: 41 years
Weight Lost: 31 lbs (from 190 lbs to 159 lbs)
Total Inches Lost: 22 inches (from 242 inches to 220 inches)
Weight Lost: 31 lbs (from 190 lbs to 159 lbs)
Total Inches Lost: 22 inches (from 242 inches to 220 inches)
Finalist #4 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #5
Lost 22 lbs and 13 total inches!
Age: 37 years
Weight Lost: 22 lbs (from 172 lbs to 150 lbs)
Total Inches Lost: 13 inches (from 230 inches to 217 inches)
Weight Lost: 22 lbs (from 172 lbs to 150 lbs)
Total Inches Lost: 13 inches (from 230 inches to 217 inches)
Finalist #5 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #6
Lost 120 lbs and 77 total inches!
Age: 40 years
Weight Lost: 120 lbs (from 359 lbs to 239 lbs)
Total Inches Lost: 77 inches (from 331 inches to 254 inches)
Weight Lost: 120 lbs (from 359 lbs to 239 lbs)
Total Inches Lost: 77 inches (from 331 inches to 254 inches)
Finalist #6 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #7
Lost 48 lbs and 36 total inches!
Age: 42 years
Weight Lost: 48 lbs (from 242 lbs to 194 lbs)
Total Inches Lost: 36 inches (from 268 inches to 232 inches)
Weight Lost: 48 lbs (from 242 lbs to 194 lbs)
Total Inches Lost: 36 inches (from 268 inches to 232 inches)
Finalist #7 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #8
Lost 46 lbs and 37 total inches!
Age: 36 years
Weight Lost: 46 lbs (from 209 lbs to 163 lbs)
Total Inches Lost: 37 inches (from 246 inches to 209 inches)
Weight Lost: 46 lbs (from 209 lbs to 163 lbs)
Total Inches Lost: 37 inches (from 246 inches to 209 inches)
Finalist #8 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #9
Lost 25 lbs and 14 total inches!
Age: 49 years
Weight Lost: 25 lbs (from 228 lbs to 203 lbs)
Total Inches Lost: 14 inches (from 246 inches to 232 inches)
Weight Lost: 25 lbs (from 228 lbs to 203 lbs)
Total Inches Lost: 14 inches (from 246 inches to 232 inches)
Finalist #9 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #10
Lost 47 lbs and 28 total inches!
Age: 39 years
Weight Lost: 47 lbs (from 263 lbs to 216 lbs)
Total Inches Lost: 28 inches (from 265 inches to 237 inches)
Weight Lost: 47 lbs (from 263 lbs to 216 lbs)
Total Inches Lost: 28 inches (from 265 inches to 237 inches)
Finalist #10 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #11
Lost 41 lbs and 35 total inches!
Age: 40 years
Weight Lost: 41 lbs (from 319 lbs to 278 lbs)
Total Inches Lost: 35 inches (from 298 inches to 263 inches)
Weight Lost: 41 lbs (from 319 lbs to 278 lbs)
Total Inches Lost: 35 inches (from 298 inches to 263 inches)
Finalist #11 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #12

Lost 44 lbs and 26 total inches!
Age: 38 years
Weight Lost: 44 lbs (from 226 lbs to 182 lbs)
Total Inches Lost: 26 inches (from 259 inches to 233 inches)
Weight Lost: 44 lbs (from 226 lbs to 182 lbs)
Total Inches Lost: 26 inches (from 259 inches to 233 inches)
Finalist #12 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #13
Lost 22 lbs and 10 total inches!
Age: 69 years
Weight Lost: 22 lbs (from 200 lbs to 178 lbs)
Total Inches Lost: 10 inches (from 233 inches to 223 inches)
Weight Lost: 22 lbs (from 200 lbs to 178 lbs)
Total Inches Lost: 10 inches (from 233 inches to 223 inches)
Finalist #13 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #14
Lost 44 lbs and 23 total inches!
Age: 38 years
Weight Lost: 44 lbs (from 253 lbs to 209 lbs)
Total Inches Lost: 23 inches (from 269 inches to 246 inches)
Weight Lost: 44 lbs (from 253 lbs to 209 lbs)
Total Inches Lost: 23 inches (from 269 inches to 246 inches)
Finalist #14 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #15

Lost 43 lbs and 24 total inches!
Age: 40 years
Weight Lost: 43 lbs (from 276 lbs to 233 lbs)
Total Inches Lost: 24 inches (from 275 inches to 251 inches)
Weight Lost: 43 lbs (from 276 lbs to 233 lbs)
Total Inches Lost: 24 inches (from 275 inches to 251 inches)
Finalist #15 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #16
Lost 57 lbs and 20 total inches!
Age: 40 years
Weight Lost: 57 lbs (from 362 lbs to 305 lbs)
Total Inches Lost: 20 inches (from 306 inches to 286 inches)
Weight Lost: 57 lbs (from 362 lbs to 305 lbs)
Total Inches Lost: 20 inches (from 306 inches to 286 inches)
Finalist #16 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #17

Lost 24 lbs and 18 total inches!
Age: 35 years
Weight Lost: 24 lbs (from 208 lbs to 184 lbs)
Total Inches Lost: 18 inches (from 244 inches to 226 inches)
Weight Lost: 24 lbs (from 208 lbs to 184 lbs)
Total Inches Lost: 18 inches (from 244 inches to 226 inches)
Finalist #17 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #18

Lost 11 lbs and 4 total inches!
Age: 35 years
Weight Lost: 11 lbs (from 187 lbs to 176 lbs)
Total Inches Lost: 4 inches (from 225 inches to 221 inches)
Weight Lost: 11 lbs (from 187 lbs to 176 lbs)
Total Inches Lost: 4 inches (from 225 inches to 221 inches)
Finalist #18 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #19

Lost 17 lbs and 11 total inches!
Age: 42 years
Weight Lost: 17 lbs (from 175 lbs to 158 lbs)
Total Inches Lost: 11 inches (from 221 inches to 210 inches)
Weight Lost: 17 lbs (from 175 lbs to 158 lbs)
Total Inches Lost: 11 inches (from 221 inches to 210 inches)
Finalist #19 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #20
Gained 10 lbs and 11 total inches!

- Age: 25 years
- Weight Gained: 10 lbs (from 187 lbs to 197 lbs)
- Total Inches Gained: 11 inches (from 224 inches to 235 inches)
-

Finalist #20 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Confirm your choice for the Men’s $25,000 Grand Prize winner
When confirming your vote, it’s important to remember that we’re not rewarding the best bodies per se. We’re rewarding the most incredible transformations.
In Precision Nutrition Coaching, we certainly don’t expect folks to start off looking like fitness models. Heck, we don’t even expect folks to end up looking like fitness models.
We’re looking for winners who’ve made the most dramatic changes in their own bodies, starting from wherever they were at the beginning.
That’s because our coaching is for men and women of all shapes and sizes. And your vote should reflect who you think achieved the most dramatic changes over the last 12 months.
Want to transform your body just like these men did?
Most people know that regular movement, eating well, sleep, and stress management are important for looking and feeling better. Yet they need help applying that knowledge in the context of their busy, sometimes stressful lives.
Over the past 15 years, we’ve used the Precision Nutrition Coaching method to help over 100,000 clients lose fat, get stronger, and improve their health… for the long-term… no matter what challenges they’re dealing with.
It’s also why we work with health, fitness, and wellness professionals (through our Level 1 and Level 2 Certification programs) to teach them how to coach their own clients through the same challenges.
Interested in Precision Nutrition Coaching? Join the presale list; you’ll save up to 54% and secure a spot 24 hours early.
We’ll be opening up spots in our next Precision Nutrition Coaching on Wednesday, January 15th, 2020.
If you’re interested in coaching and want to find out more, I’d encourage you to join our presale list below. Being on the list gives you two special advantages.
- You’ll pay less than everyone else. At Precision Nutrition we like to reward the most interested and motivated people because they always make the best clients. Join the presale list and you’ll save up to 54% off the general public price, which is the lowest price we’ve ever offered.
- You’re more likely to get a spot. To give clients the personal care and attention they deserve, we only open up the program twice a year. Last time we opened registration, we sold out within minutes. By joining the presale list you’ll get the opportunity to register 24 hours before everyone else, increasing your chances of getting in.
If you’re ready to change your body, and your life, with help from the world’s best coaches, this is your chance.
[Note: If your health and fitness are already sorted out, but you’re interested in helping others, check out our Precision Nutrition Level 1 Certification program].
The post Precision Nutrition Coaching: January 2020 Men’s Finalists. Help us give away $125,000! appeared first on Precision Nutrition.
Source: Health1
Only a year ago, these 20 women were feeling frustrated. They were inspired to eat healthier, move better, and feel stronger… but unsure how to make a change that would really stick.
Now, after just 12 months of Precision Nutrition Coaching, they’ve taken control of their health and fitness for good—transforming their health, bodies, and lives more than they ever thought possible. Eating healthier and living an active lifestyle is now second nature. Something they do without stress and anxiety, and without feeling pressure to be perfect all the time.
They also have the chance to take home part of the $125,000 in prize money we’ve once again committed to our latest round of top clients. Scroll through these amazing photos and vote for the finalist whose transformation inspires you most.
++
Every year in Precision Nutrition Coaching, we help men and women from around the world dramatically improve their eating habits, exercise routine, and lifestyle.
With a world-class coach guiding and supporting them every step of the way, they lose weight, gain strength, and completely transform their bodies, health, fitness, and lives.
We also give clients a big, motivating goal to shoot for: $250,000 in cash prizes.
Consider it an antidote to the “you must suffer and feel guilty to get in shape” message you typically get from the fitness industry.
See, women come to us wanting big changes:
- They want to lose weight and shed body fat.
- They want to gain strength and/or lean mass.
- They want to make healthier food choices, consistently.
- They want to feel at ease, instead of stressed out, around food.
- They want to feel confident and comfortable in their own skin.
- They want to start doing all the awesome things they’ve always wanted to do, but thought they couldn’t.
Above all, they want to become the fittest, strongest, healthiest versions of themselves.
In our experience, big, inspiring, life-changing goals like these are a whole lot easier to achieve when there’s a huge bonus at stake.
So, every six months, we divvy up a big pot of prize money for the best transformations among our male and female clients.
For the current group—which started in January 2019 and is wrapping up now—we’ve committed $125,000.
And right now, we need your help to choose our Women’s Grand Prize winner.
Help choose our Women’s Grand Prize winner (Top prize = $25,000)
The women below started their Precision Nutrition Coaching journey in all shapes and sizes, and they hail from all parts of the globe.
As moms, partners, daughters, employees, students, siblings, caretakers—or some combination thereof—they’d spent a good deal of their time helping and caring for others. And they were ready to take care of themselves and start living their best life.
They’re a diverse group with one thing in common: Now, after just 12 months of Precision Nutrition Coaching, they have the bodies and health they’ve wanted for a long time, and they’re confident they’ll stay this way for good.
How’d they do it?
No crash diets. No Biggest Loser-type bootcamps. And no full-time chefs.
Just research-based nutrition and lifestyle habits practiced daily—and personalized help from our expert coaches.
To vote for the woman you think should win the $25,000 Grand Prize, scroll through the photos below. Make your choice by clicking the “Vote for Finalist” button under the one you think achieved the best transformation.
But please don’t stop there. Once you’ve seen all the finalists and selected your #1 choice, scroll down to the bottom of this post.
At the bottom you’ll need to verify your choice. To do this, click the “Place your vote” button. This will log your vote and help us make our decision.
Thanks for your help!
Finalist #1
Lost 27 lbs and 25 total inches!
Age: 59 years
Weight Lost: 27 lbs (from 187 lbs to 160 lbs)
Total Inches Lost: 25 inches (from 216 inches to 191 inches)
Weight Lost: 27 lbs (from 187 lbs to 160 lbs)
Total Inches Lost: 25 inches (from 216 inches to 191 inches)
Finalist #1 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #2
Lost 21 lbs and 20 total inches!
Age: 39 years
Weight Lost: 21 lbs (from 154 lbs to 133 lbs)
Total Inches Lost: 20 inches (from 219 inches to 199 inches)
Weight Lost: 21 lbs (from 154 lbs to 133 lbs)
Total Inches Lost: 20 inches (from 219 inches to 199 inches)
Finalist #2 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #3
Lost 34 lbs and 29 total inches!
Age: 37 years
Weight Lost: 34 lbs (from 159 lbs to 125 lbs)
Total Inches Lost: 29 inches (from 229 inches to 200 inches)
Weight Lost: 34 lbs (from 159 lbs to 125 lbs)
Total Inches Lost: 29 inches (from 229 inches to 200 inches)
Finalist #3 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #4
Lost 44 lbs and 37 total inches!
Age: 53 years
Weight Lost: 44 lbs (from 158 lbs to 114 lbs)
Total Inches Lost: 37 inches (from 220 inches to 183 inches)
Weight Lost: 44 lbs (from 158 lbs to 114 lbs)
Total Inches Lost: 37 inches (from 220 inches to 183 inches)
Finalist #4 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #5
Lost 20 lbs and 18 total inches!
Age: 65 years
Weight Lost: 20 lbs (from 147 lbs to 127 lbs)
Total Inches Lost: 18 inches (from 204 inches to 186 inches)
Weight Lost: 20 lbs (from 147 lbs to 127 lbs)
Total Inches Lost: 18 inches (from 204 inches to 186 inches)
Finalist #5 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #6
Lost 45 lbs and 42 total inches!
Age: 46 years
Weight Lost: 45 lbs (from 165 lbs to 120 lbs)
Total Inches Lost: 42 inches (from 228 inches to 186 inches)
Weight Lost: 45 lbs (from 165 lbs to 120 lbs)
Total Inches Lost: 42 inches (from 228 inches to 186 inches)
Finalist #6 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #7
Lost 27 lbs and 11 total inches!
Age: 40 years
Weight Lost: 27 lbs (from 173 lbs to 146 lbs)
Total Inches Lost: 11 inches (from 221 inches to 210 inches)
Weight Lost: 27 lbs (from 173 lbs to 146 lbs)
Total Inches Lost: 11 inches (from 221 inches to 210 inches)
Finalist #7 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #8
Lost 18 lbs and 20 total inches!
Age: 55 years
Weight Lost: 18 lbs (from 154 lbs to 136 lbs)
Total Inches Lost: 20 inches (from 222 inches to 202 inches)
Weight Lost: 18 lbs (from 154 lbs to 136 lbs)
Total Inches Lost: 20 inches (from 222 inches to 202 inches)
Finalist #8 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #9
Lost 32 lbs and 24 total inches!
Age: 25 years
Weight Lost: 32 lbs (from 199 lbs to 167 lbs)
Total Inches Lost: 24 inches (from 236 inches to 212 inches)
Weight Lost: 32 lbs (from 199 lbs to 167 lbs)
Total Inches Lost: 24 inches (from 236 inches to 212 inches)
Finalist #9 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #10

Lost 13 lbs and 10 total inches!
Age: 68 years
Weight Lost: 13 lbs (from 157 lbs to 144 lbs)
Total Inches Lost: 10 inches (from 222 inches to 212 inches)
Weight Lost: 13 lbs (from 157 lbs to 144 lbs)
Total Inches Lost: 10 inches (from 222 inches to 212 inches)
Finalist #10 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #11
Lost 20 lbs and 40 total inches!
Age: 38 years
Weight Lost: 20 lbs (from 190 lbs to 170 lbs)
Total Inches Lost: 40 inches (from 244 inches to 204 inches)
Weight Lost: 20 lbs (from 190 lbs to 170 lbs)
Total Inches Lost: 40 inches (from 244 inches to 204 inches)
Finalist #11 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #12
Lost 24 lbs and 21 total inches!
Age: 37 years
Weight Lost: 24 lbs (from 145 lbs to 121 lbs)
Total Inches Lost: 21 inches (from 204 inches to 183 inches)
Weight Lost: 24 lbs (from 145 lbs to 121 lbs)
Total Inches Lost: 21 inches (from 204 inches to 183 inches)
Finalist #12 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #13
Lost 12 lbs and 14 total inches!
Age: 59 years
Weight Lost: 12 lbs (from 126 lbs to 114 lbs)
Total Inches Lost: 14 inches (from 207 inches to 193 inches)
Weight Lost: 12 lbs (from 126 lbs to 114 lbs)
Total Inches Lost: 14 inches (from 207 inches to 193 inches)
Finalist #13 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #14
Lost 27 lbs and 30 total inches!
Age: 38 years
Weight Lost: 27 lbs (from 175 lbs to 148 lbs)
Total Inches Lost: 30 inches (from 224 inches to 194 inches)
Weight Lost: 27 lbs (from 175 lbs to 148 lbs)
Total Inches Lost: 30 inches (from 224 inches to 194 inches)
Finalist #14 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #15
Lost 40 lbs and 36 total inches!
Age: 57 years
Weight Lost: 40 lbs (from 227 lbs to 187 lbs)
Total Inches Lost: 36 inches (from 267 inches to 231 inches)
Weight Lost: 40 lbs (from 227 lbs to 187 lbs)
Total Inches Lost: 36 inches (from 267 inches to 231 inches)
Finalist #15 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #16
Lost 15 lbs and 16 total inches!
Age: 47 years
Weight Lost: 15 lbs (from 141 lbs to 126 lbs)
Total Inches Lost: 16 inches (from 216 inches to 200 inches)
Weight Lost: 15 lbs (from 141 lbs to 126 lbs)
Total Inches Lost: 16 inches (from 216 inches to 200 inches)
Finalist #16 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #17

Lost 12 lbs and 13 total inches!
Age: 42 years
Weight Lost: 12 lbs (from 143 lbs to 131 lbs)
Total Inches Lost: 13 inches (from 212 inches to 199 inches)
Weight Lost: 12 lbs (from 143 lbs to 131 lbs)
Total Inches Lost: 13 inches (from 212 inches to 199 inches)
Finalist #17 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #18

Lost 18 lbs and 19 total inches!
Age: 36 years
Weight Lost: 18 lbs (from 159 lbs to 141 lbs)
Total Inches Lost: 19 inches (from 216 inches to 197 inches)
Weight Lost: 18 lbs (from 159 lbs to 141 lbs)
Total Inches Lost: 19 inches (from 216 inches to 197 inches)
Finalist #18 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #19

Lost 14 lbs and 23 total inches!
Age: 45 years
Weight Lost: 14 lbs (from 162 lbs to 148 lbs)
Total Inches Lost: 23 inches (from 227 inches to 204 inches)
Weight Lost: 14 lbs (from 162 lbs to 148 lbs)
Total Inches Lost: 23 inches (from 227 inches to 204 inches)
Finalist #19 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Finalist #20

Lost 15 lbs and 21 total inches!
Age: 38 years
Weight Lost: 15 lbs (from 135 lbs to 120 lbs)
Total Inches Lost: 21 inches (from 202 inches to 181 inches)
Weight Lost: 15 lbs (from 135 lbs to 120 lbs)
Total Inches Lost: 21 inches (from 202 inches to 181 inches)
Finalist #20 selected!
After reviewing all the finalists – you can change your vote at any time – click “Place your vote” at the bottom of this page to record your choice.
Confirm your choice for the Women’s $25,000 Grand Prize winner
When confirming your vote, it’s important to remember that we’re not rewarding the best bodies per se. We’re rewarding the most incredible transformations.
In Precision Nutrition Coaching, we certainly don’t expect folks to start off looking like fitness models. Heck, we don’t even expect folks to end up looking like fitness models.
We’re looking for winners who’ve made the most dramatic changes in their own bodies, starting from wherever they were at the beginning.
That’s because our coaching is for men and women of all shapes and sizes. And your vote should reflect who you think achieved the most dramatic changes over the last 12 months.
Note: There is a poll embedded within this post, please visit the site to participate in this post’s poll.
Want to transform your body like these women did?
Most people know that regular movement, eating well, sleep, and stress management are important for getting the body and health they want. Yet they need help applying that knowledge in the context of their busy, sometimes stressful lives.
Over the past 15 years, we’ve used the Precision Nutrition Coaching method to help over 100,000 clients lose fat, get stronger, and improve their health… for the long-term… no matter what challenges they’re dealing with.
It’s also why we work with health, fitness, and wellness professionals (through our Level 1 and Level 2 Certification programs) to teach them how to coach their own clients through the same challenges.
Interested in Precision Nutrition Coaching? Join the presale list; you’ll save up to 54% and secure a spot 24 hours early.
We’ll be opening up spots in our next Precision Nutrition Coaching on Wednesday, January 15th, 2020.
If you’re interested in coaching and want to find out more, I’d encourage you to join our presale list below. Being on the list gives you two special advantages.
- You’ll pay less than everyone else. At Precision Nutrition we like to reward the most interested and motivated people because they always make the best clients. Join the presale list and you’ll save up to 54% off the general public price, which is the lowest price we’ve ever offered.
- You’re more likely to get a spot. To give clients the personal care and attention they deserve, we only open up the program twice a year. Last time we opened registration, we sold out within minutes. By joining the presale list you’ll get the opportunity to register 24 hours before everyone else, increasing your chances of getting in.
If you’re ready to change your body, and your life, with help from the world’s best coaches, this is your chance.
[Note: If your health and fitness are already sorted out, but you’re interested in helping others, check out our Precision Nutrition Level 1 Certification program].
The post Precision Nutrition Coaching: January 2020 Women’s Finalists. Help us give away $125,000! appeared first on Precision Nutrition.
Source: Health1
Tired of so-called “experts” telling you how to eat better and improve your fitness? If so, this article is your antidote. In it we share 35 tips, ideas, and strategies that actual clients—folks like you—have used to get into the best shape of their lives.
++++
Imagine a life where you…
…feel physically and mentally strong, capable of taking on any challenge without worrying that your energy levels or bodyweight will get in the way.
…can run around with your kids, or grandkids, without feeling pain, winded, or tired; and you can do it again the next day.
…excitedly book a beach vacation without wondering how you’ll look (or feel) in a swimsuit, walking along the beach.
…look forward to having your picture taken without wondering “who’s that person, and when did they start looking like that?”
It’s not a pipe dream.
Here at Precision Nutrition, we’ve worked with thousands of clients and heard their deepest reasons for wanting to change their bodies and their lives.
(You’ll read about some of them below, you’ll even see some of their photos).
Strange as it’ll seem, most of them didn’t believe change was really possible. Not within the context of their uniquely busy, often stressful lives.
When they started working with us, their goals seemed more like fantasies. Even the simple ones—like wanting to get up off the floor without having to say “umphhhh”—felt out of reach.
But notice what happened next.
They lost body weight and fat. They built strength. The reclaimed their health. And they took control of their fitness, some for the first time in their lives.
Nowadays they’re the women you see projecting confidence and walking tall. The men with flat stomachs and a totally clean bill of health.
So we decided to ask them:
How’d you do it?
Their real-world answers were so good we decided to share them today.
In this article you’ll learn:
- The common obstacles many of our clients face.
- The fears many of them felt when starting out.
- How they overcame their fears, got past their obstacles.
- And how you can do the same.
Before getting into it, though, I wanted to let you know that we’re soon opening spots in our Precision Nutrition Coaching program.
You see, twice a year we work with small groups of men and women interested in looking and feeling better. Over the course of 12 months we help them get into the best shape of their lives… and stay that way for good.
Just so you know, we’ve tested Precision Nutrition Coaching with close to over 100,000 clients over the past 15 years. Plus, several peer-reviewed research papers have documented the safety and effectiveness of our approach.
For a sneak peek at the amazing things we’ve helped them accomplish, check out this short video:
Meet some of the people whose bodies—and lives—have been changed by Precision Nutrition Coaching.
Wondering how you can experience these kinds of results for yourself?
Let’s turn it over to our Precision Nutrition Coaching graduates.
Having trouble getting started?
Don’t think, just do.
“If it’s your time, and you’re sitting on the fence—you want to do it, you’re thinking of doing it, you’re not sure if you should do it—jump off that fence,” says Patrick, 35, who lost 152 pounds with Precision Nutrition.
“Give it everything you’ve got; why sit out when you can be part of life?”
Patrick’s Transformation

Lost 152 lbs and 20% body fat!
Age: 35 years
Weight Lost: 152 lbs (from 417 lbs to 265 lbs)
% Body Fat Lost: 20% (from 39.1% to 19.1%)
Total Inches Lost: 73 inches (from 337 inches to 264 inches)
Weight Lost: 152 lbs (from 417 lbs to 265 lbs)
% Body Fat Lost: 20% (from 39.1% to 19.1%)
Total Inches Lost: 73 inches (from 337 inches to 264 inches)
Turned off by every weight-loss program and tip you see?
Ignore mainstream advice.
Unrealistic (and, frankly, insulting) click bait like “Flatten Your Tummy in 5 Minutes a Day” and “Sculpt Your Butt While Sitting Still” are meant to drive ad sales, not get you in shape.
Most of our clients, once they see Precision Nutrition’s positive, practice-based approach, realize that the negative tone of health and fitness media was holding them back for years.
Find trustworthy friends or acquaintances who lost weight, and do what they did.
Why reinvent the wheel? When you see a true success story unfold before your eyes, copycat away. That’s how 46-year-old Sharon D’Arcy found Precision Nutrition, and she ended up losing more than 30 pounds.
(Click here for her story, which includes a bit of surprising inspiration.)
Sharon’s Transformation

Lost 33 lbs and 13% body fat!
Age: 46 years
Weight Lost: 33 lbs (from 151 lbs to 118 lbs)
% Body Fat Lost: 13% (from 28% to 15%)
Total Inches Lost: 18.5 inches (from 209.1 inches to 190.6 inches)
Weight Lost: 33 lbs (from 151 lbs to 118 lbs)
% Body Fat Lost: 13% (from 28% to 15%)
Total Inches Lost: 18.5 inches (from 209.1 inches to 190.6 inches)
Make it about your journey.
Don’t assume you have to be “perfect” or “special” in order to be fit and healthy. 48-year-old Alicia had been on the diet-mobile for so long she started to think change just wasn’t possible for her.
Then one day, her mindset shifted. “Why not me?” she asked herself. She stuck that mantra to her mirror.
Every day, in a mindful, conscious way, she visualized her success. Forty-nine pounds later, Alicia went from a size 16 to a size 6 and became our $25,000 grand prize winner.
Alicia’s Transformation

Lost 49 lbs and 46 total inches!
Age: 48 years
Weight Lost: 49 lbs (from 181 lbs to 132 lbs)
Total Inches Lost: 46 inches (from 219 inches to 173 inches)
Weight Lost: 49 lbs (from 181 lbs to 132 lbs)
Total Inches Lost: 46 inches (from 219 inches to 173 inches)
Struggling to get motivated and inspired?
Stop living in “coulda, woulda, shoulda”.
To make true progress, allow yourself to focus exclusively on what you can do now. Not in some hypothetical future where everything is perfect.
Just do the best you can with what you’ve got right now. It’s what allowed Sharon (above) to lose weight and fight cancer—all in the same year.
Have your reason.
Keep your specific motivation in mind, whether it’s getting fit enough to play sports with your kids or looking great on your wedding day. That last one is what helped 32-year-old Melissa lose 55 pounds.
“The whole time, I had this image of myself on my wedding day in my head,” Melissa says. “Walking tall, feeling amazing—feeling statuesque instead of soft around the edges.”
Melissa’s Transformation

Lost 55 lbs and 16% body fat!
Age: 32 years
Weight Lost: 55 lbs (from 231 lbs to 176 lbs)
% Body Fat Lost: 16% (from 34% to 18%)
Total Inches Lost: 38 inches (from 242 inches to 204 inches)
Weight Lost: 55 lbs (from 231 lbs to 176 lbs)
% Body Fat Lost: 16% (from 34% to 18%)
Total Inches Lost: 38 inches (from 242 inches to 204 inches)
Feel more than you see.
Sure, wanting to look better is what motivates most clients to sign up for Precision Nutrition Coaching. But it’s not what gets them to oh-my-god-you-look-amazing transformations.
Healthy eating habits end up improving how they feel—how they move, think and generally enjoy life—which leads to continued healthy eating and dozens of pounds lost over time.
Focus on the joy of movement.
“Enjoy your body,” Sharon (above) says. “Take pleasure in movement. Take pride in what you can do.”
This deep appreciation for physical health is what allows many clients to maintain fitness regimens and weight loss over time.
Recognize true enjoyment.
Most Precision Nutrition clients come to realize that they’ve been eating mindlessly—packing in calories without really tasting the food—for a long time.
“There’s nothing inherently wrong with dessert,” explains Yano, 35, who lost 76 pounds with Precision Nutrition.
He still enjoys dessert occasionally, of course, and finds that having it only once in awhile is the key to really appreciating it.
Yano’s Transformation
Lost 76 lbs and 20.9% body fat!
Age: 35 years
Weight Lost: 76 lbs (from 256 lbs to 180 lbs)
% Body Fat Lost: 20.9% (from 34.1% to 13.2%)
Waist Inches Lost: 10 inches (from 43 inches to 33 inches)
Weight Lost: 76 lbs (from 256 lbs to 180 lbs)
% Body Fat Lost: 20.9% (from 34.1% to 13.2%)
Waist Inches Lost: 10 inches (from 43 inches to 33 inches)
Feel like the ‘real you’ has gotten lost somewhere along the way?
Pay attention to your environment.
Recognizing how their surroundings might have caused unhealthy habits to develop—like 29-year-old Sarah’s years of work in fast food restaurants—allows many Precision Nutrition clients to discover the why of who they are and start zeroing in on the power of how to change it.
Sarah’s Transformation

Lost 52 lbs and 14.2% body fat!
Age: 29 years
Weight Lost: 52 lbs (from 191 lbs to 139 lbs)
% Body Fat Lost: 14.2% (from 26.3% to 12.1%)
Total Inches Lost: 50 inches (from 239 inches to 189 inches)
Weight Lost: 52 lbs (from 191 lbs to 139 lbs)
% Body Fat Lost: 14.2% (from 26.3% to 12.1%)
Total Inches Lost: 50 inches (from 239 inches to 189 inches)
Don’t fall to pack mentality.
“It turns out that a lot of people have health and weight issues, just like I used to have,” Yano (above) says.
“And often they don’t want to eat poorly; they just do it because everyone else—friends, family, the people around them—is doing it. That was my problem for a long time.”
Dive below the surface.
We can skim the top of our diet issues and see some small, fleeting changes on the scale… or we can really dig into our relationship with food, and make it better for the long run.
For Sarah (above), letting herself get vulnerable as she went through Precision Nutrition’s program turned into her greatest strength, opening her up to the process of self-questioning:
“How have trying times brought me to where I am now, and how have I coped?” Sarah asked herself. “What do I really care about? What gives me joy? How can I get more of that?”
Along the way, Sarah lost 52 pounds.
Say goodbye to the old you.
This isn’t some meaningless cliché. We’ve found that many people harbor an invisible fear of losing themselves if they lose a bunch of weight.
Consciously mourn your old self as you greet the healthier you. Lots of Precision Nutrition clients were able to recognize and minimize certain anxieties this way.
Stay connected to what you love about yourself.
“Just remember, you deserve all of the amazing insights, strength gains, friendships, learning—whatever you take from this program as you find and discover a new and best version of yourself,” Sarah (above) says.
“You are worthy.”
Exhausted just thinking about how much work you’ll have to do?
Know that everyone—everyone—has to work at it.
Fit, healthy people who look like they’ve got it all figured out have to put effort into eating right, too.
We know because Precision Nutrition coaches themselves talk about it a lot.
Clients say getting to know them is comforting, because you can see how they’re so focused on learning, growing, and becoming the best versions of themselves.
De-emphasize the “work” in “working out”.
So many Precision Nutrition clients say that one outcome of our program—and something that helps them maintain an optimal exercise schedule—is coming to see movement as play, as fun, as release.
Find the activities you love, and moving your body will become something you seek out, not dread.
Let it be easy.
Like many Precision Nutrition clients, 34-year-old Chrystalene used to beat herself up when she failed, and thought she should be able to get fit without a speck of help.
Luckily, through Precision Nutrition Coaching, she learned, “it doesn’t have to be hard all the time. And it’s okay to seek support. There’s probably a way to make your heavy thing lighter, and finding out how to do that is worth it.”
Her results—86 pounds lost and a $25,000 Grand Prize from Precision Nutrition—show what’s possible when you relax a little, and lean on the people around you.
Chrystalene’s Transformation

Lost 86 lbs and 55 total inches!
Age: 34 years
Weight Lost: 86 lbs (from 259 lbs to 173 lbs)
Total Inches Lost: 55 inches (from 269 inches to 214 inches)
Weight Lost: 86 lbs (from 259 lbs to 173 lbs)
Total Inches Lost: 55 inches (from 269 inches to 214 inches)
Swap “comparison” for inspiration.
Forget envy and intimidation. Precision Nutrition clients notice that the program allows them to stop saying, “That could never be me” and start thinking of others’ success stories as inspiration.
Lots of Precision Nutrition clients come to the program with significant health issues to solve. Talk to them and let their energy fuel you.
Just take small steps every day
It’s easy to think you have to make all of the changes, all at once. But small steps really do add up.
That’s what 51-year-old Mark—who lost 42 pounds and won a $25,000 Grand Prize—learned from Precision Nutrition Coaching.
Says Mark, “Be patient. Just show up every day and focus on making small changes consistently”.
Mark’s Transformation

Lost 42 lbs and 32 total inches!
Age: 51 years
Weight Lost: 42 lbs (from 192 lbs to 150 lbs)
Total Inches Lost: 32 inches (from 237 inches to 205 inches)
Weight Lost: 42 lbs (from 192 lbs to 150 lbs)
Total Inches Lost: 32 inches (from 237 inches to 205 inches)
Know a lot about health and nutrition, but can’t seem to change?
Redefine “knowing”.
“It’s about realizing that no matter how smart I am and how much I know about exercise, if I’m not living it, I don’t really know it,” says Kevin, 40, who lost 37 pounds on the Precision Nutrition program.
Kevin’s Transformation

Lost 37 lbs and 12.8% body fat!
Age: 40 years
Weight Lost: 37 lbs (from 177 lbs to 140 lbs)
% Body Fat Lost: 12.8% (from 20.1% to 7.3%)
Waist Inches Lost: 21 inches (from 226 inches to 205 inches)
Weight Lost: 37 lbs (from 177 lbs to 140 lbs)
% Body Fat Lost: 12.8% (from 20.1% to 7.3%)
Waist Inches Lost: 21 inches (from 226 inches to 205 inches)
Let others take the helm.
Many Precision Nutrition clients know a whole lot about health and nutrition coming into our program. In fact, a lot of them are fitness instructors and health professionals themselves. Why’s the weight still sticking to them?
Their lightbulb moment: Relinquishing control to coaches, who offer the practical lifestyle advice, daily habits, and—this is key—accountability that’s needed to create real change.
Find your route at the grocery store.
“Knowing” is not always the same as “doing”. So many people trying to “eat clean” get derailed by the mere sight of processed food.
Precision Nutrition clients learn how to navigate the supermarket (or restaurants or their workplaces) to avoid temptation.
The secret: Stay on the perimeter. Calorie-packed chips, cookies, pasta, sauces, and dressings are in the middle. The good stuff like vegetables, meats, eggs, and fruits are stocked on the outside, away from the aisles.
That’s what 46-year-old John learned, and he lost 106 pounds.
John’s Transformation
Lost 106 lbs and 13% body fat!
Age: 46 years
Weight Lost: 106 lbs (from 332 lbs to 226 lbs)
% Body Fat Lost: 13% (from 39% to 26%)
Waist Inches Lost: 12 inches (from 50 inches to 38 inches)
Weight Lost: 106 lbs (from 332 lbs to 226 lbs)
% Body Fat Lost: 13% (from 39% to 26%)
Waist Inches Lost: 12 inches (from 50 inches to 38 inches)
Find accountability.
“The truth is, I probably knew three-quarters of Precision Nutrition Coaching’s dietary recommendations before I started,” says Peter, 52, who dropped 33 pounds with Precision Nutrition.
“But the secret to losing weight and maintaining a healthy weight is consistency,” he says. Get someone to breathe down your neck, and you’ll make healthy choices your habit.
Peter’s Transformation

Lost 33 lbs and 11% body fat!
Age: 52 years
Weight Lost: 33 lbs (from 180 lbs to 147 lbs)
% Body Fat Lost: 11% (from 18% to 7%)
Waist Inches Lost: 5 inches (from 35 inches to 30 inches)
Weight Lost: 33 lbs (from 180 lbs to 147 lbs)
% Body Fat Lost: 11% (from 18% to 7%)
Waist Inches Lost: 5 inches (from 35 inches to 30 inches)
Can’t figure out how to work it into your busy life?
Realize there’s no such thing as “too busy”.
Precision Nutrition’s program is practically custom-designed for people who think they just “don’t have the time”. Oftentimes they’re our most successful clients.
Lisanne, 39, lost 38 pounds on the Precision Nutrition program while taking care of three small kids—including a nursing infant—and getting certified as a yoga instructor and doula.
Other clients work multiple jobs or have to travel five days a week and never know where they’ll be staying next. They tell us that Precision Nutrition coaching actually ends up easing their schedule by lending structure to their lives.
Lisanne’s Transformation

Lost 38 lbs and 14% body fat!
Age: 39 years
Weight Lost: 38 lbs (from 160 lbs to 122 lbs)
% Body Fat Lost: 14% (from 36% to 22%)
Total Inches Lost: 41 inches (from 229 inches to 188 inches)
Weight Lost: 38 lbs (from 160 lbs to 122 lbs)
% Body Fat Lost: 14% (from 36% to 22%)
Total Inches Lost: 41 inches (from 229 inches to 188 inches)
Focus on what you can do right now.
Forget what you can’t do. Figure out what you’re capable of in this moment, and build from there.
“I had to find it within me to accept that it was okay to do things a bit differently, says Richard, 49, who dropped 103 pounds in our yearlong program.
“I had to accept that it was okay to do what I was capable of.”
Eventually, Precision Nutrition clients internalize this mantra: Start wherever you are. Use whatever you have. Do whatever you can.
Richard’s Transformation

Lost 103 lbs and 20% body fat!
Age: 49 years
Weight Lost: 103 lbs (from 318 lbs to 215 lbs)
% Body Fat Lost: 20% (from 40.9% to 20.9%)
Total Inches Lost: 30 inches (from 285 inches to 255 inches)
Weight Lost: 103 lbs (from 318 lbs to 215 lbs)
% Body Fat Lost: 20% (from 40.9% to 20.9%)
Total Inches Lost: 30 inches (from 285 inches to 255 inches)
Picture the health role model you want for your kids.
Now be that.
“I want my kids to be healthy and happy and proud of the way they’re living their lives,” Lisanne (above) says. “It’s not enough for me to pay lip service to that idea—I have to be an example.”
Don’t confuse selfishness with self-love.
A lot of Precision Nutrition clients worry that prioritizing themselves will take them away from the people who need them, potentially damaging professional or personal relationships.
Then they discover that the opposite is true: Caring for themselves by addressing their diet and lifestyle makes them look and feel better—and that actually makes them more accessible and present for other people.
Stop thinking you have to dedicate your whole life to losing weight.
Sure, some of the changes you have to make to get healthy will be fundamental. But the truth is that you only need a few hours per week to build a great body.
By getting the right kind of help and following simple yet powerful daily practices, anyone can lose weight, get healthy, and feel better.
That’s what 34-year-old Kia realized, and she lost 61 pounds.
Kia’s Transformation
Lost 61 lbs and 19% body fat!
Age: 34 years
Weight Lost: 61 lbs (from 199 lbs to 138 lbs)
% Body Fat Lost: 19% (from 37% to 18%)
Total Inches Lost: 50 inches (from 252 inches to 202 inches)
Weight Lost: 61 lbs (from 199 lbs to 138 lbs)
% Body Fat Lost: 19% (from 37% to 18%)
Total Inches Lost: 50 inches (from 252 inches to 202 inches)
Sometimes get frustrated and then quit?
Recognize that progress isn’t usually a straight line.
If you’re gauging success based on how much you weigh each morning, you’re bound to give up before you can establish healthy habits or see real change.
Almost as a rule, our clients’ progress graphs look like a crazy, twisted line of progress, regress, more progress, and lessons learned along the way (we know, because our software tracks it for them so they can follow along the whole time).
A year later, dozens of pounds lost—for good. Worth the roller coaster ride, for sure.
Stop blaming external factors.
“What I learned was that I had to take responsibility for my own decisions,” says Heather, 37, who lost 47 pounds on the Precision Nutrition program.
“I had to get real with myself. I learned the difference between thinking, ‘I have to do x,’ and ‘I choose to do x,’ and ‘I’m doing x.’”
Heather’s Transformation

Lost 47 lbs and 10% body fat!
Age: 37 years
Weight Lost: 47 lbs (from 219 lbs to 172 lbs)
% Body Fat Lost: 10% (from 38% to 28%)
Total Inches Lost: 43 inches (from 253 inches to 210 inches)
Weight Lost: 47 lbs (from 219 lbs to 172 lbs)
% Body Fat Lost: 10% (from 38% to 28%)
Total Inches Lost: 43 inches (from 253 inches to 210 inches)
Make health programs bend to your needs.
Too often, people trying to get fit become discouraged because exercise and nutrition programs seem inflexible, not designed for their lives.
That’s what Precision Nutrition coaches help with. We help you build an “Owner’s Manual” of operating instructions for your life.
49-year-old Cheryl lost 68 pounds—despite the fact that she was diagnosed with degenerative disc disease partway through the Precision Nutrition program. No heavy lifting? No problem. We helped her modify the workouts.
“In some ways, the diagnosis was a relief,” Cheryl says. “At least it was okay for me to admit that I hadn’t been doing what others were doing in the gym.”
Cheryl’s Transformation

Lost 68 lbs and 20% body fat!
Age: 49 years
Weight Lost: 68 lbs (from 245 lbs to 177 lbs)
% Body Fat Lost: 20% (from 44% to 24%)
Total Inches Lost: 65 inches (from 280 inches to 215 inches)
Weight Lost: 68 lbs (from 245 lbs to 177 lbs)
% Body Fat Lost: 20% (from 44% to 24%)
Total Inches Lost: 65 inches (from 280 inches to 215 inches)
Rewrite the basics.
“When I was in the middle of it, losing weight was at the forefront of my mind; now, everything is a habit,” says 36-year-old Katey, who despite having virtually no compliance with the Precision Nutrition program for the first 90 days went on to lose an impressive 116 pounds.
The key? Allowing herself to make truly fundamental lifestyle changes. “It feels a lot more like living,” she says.
Katey’s Transformation
Lost 116 lbs and 21% body fat!
Age: 36 years
Weight Lost: 116 lbs (from 255 lbs to 139 lbs)
% Body Fat Lost: 21% (from 39% to 18%)
Total Inches Lost: 65 inches (from 260 inches to 195 inches)
Weight Lost: 116 lbs (from 255 lbs to 139 lbs)
% Body Fat Lost: 21% (from 39% to 18%)
Total Inches Lost: 65 inches (from 260 inches to 195 inches)
Don’t let one cookie derail you.
“I realized I could have a clean slate every time I ‘messed up’ because this was about my healthy lifestyle, and not just a diet,” says Patricia, 46, who lost 69 pounds with Precision Nutrition.
“Precision Nutrition Coaching taught me habits and changed the way I view my body and the food I put in it. It’s a life plan, and it’s something I know I can manage forever.”
Patricia’s Transformation
Lost 69 lbs and 25% body fat!
Age: 46 years
Weight Lost: 69 lbs (from 250 lbs to 181 lbs)
% Body Fat Lost: 25% (from 50% to 25%)
Total Inches Lost: 35 inches (from 250 inches to 215 inches)
Weight Lost: 69 lbs (from 250 lbs to 181 lbs)
% Body Fat Lost: 25% (from 50% to 25%)
Total Inches Lost: 35 inches (from 250 inches to 215 inches)
Don’t expect unbroken enthusiasm.
Look, at times it’s a slog—and that’s true for everyone.
“I learned that sometimes you have to drag your ass to the gym, even if you don’t feel like going, and it was a huge burden that got lifted off me,” says Kim, 25, who lost 24 pounds with Precision Nutrition.
“And while the workout may be slow moving and uninspired at first, once you’re there it’s super easy to finish.”
Kim’s Transformation

Lost 24 lbs and 16.3% body fat!
Age: 25 years
Weight Lost: 24 lbs (from 160 lbs to 136 lbs)
% Body Fat Lost: 16.3% (from 29.5% to 13.2%)
Weight Lost: 24 lbs (from 160 lbs to 136 lbs)
% Body Fat Lost: 16.3% (from 29.5% to 13.2%)
Remember that change can catch you by surprise.
42-year-old Javier lost 60 pounds and took home a $25,000 grand prize at the end of his Precision Nutrition Coaching program.
Yet, until he saw his final photos, he did not fully recognize the change he had undergone.
In fact, just a few weeks before the photoshoot he was threatening to quit, and it was only the encouragement of his coach that kept him going.
Javier’s lesson: “remember that the road to success is paved with failures.”
Javier’s Transformation

Lost 60 lbs and 32 total inches!
Age: 42 years
Weight Lost: 60 lbs (from 245 lbs to 185 lbs)
Total Inches Lost: 32 inches (from 269 inches to 237 inches)
Weight Lost: 60 lbs (from 245 lbs to 185 lbs)
Total Inches Lost: 32 inches (from 269 inches to 237 inches)
Want help becoming the healthiest, fittest, strongest version of you?
Most people know that regular movement, eating well, sleep, and stress management are important for looking and feeling better. Yet they need help applying that knowledge in the context of their busy, sometimes stressful lives.
Over the past 15 years, we’ve used the Precision Nutrition Coaching method to help over 100,000 clients lose fat, get stronger, and improve their health… for the long-term… no matter what challenges they’re dealing with.
It’s also why we work with health, fitness, and wellness professionals (through our Level 1 and Level 2 Certification programs) to teach them how to coach their own clients through the same challenges.
Interested in Precision Nutrition Coaching? Join the presale list; you’ll save up to 54% and secure a spot 24 hours early.
We’ll be opening up spots in our next Precision Nutrition Coaching on Wednesday, January 15th, 2020.
If you’re interested in coaching and want to find out more, I’d encourage you to join our presale list below. Being on the list gives you two special advantages.
- You’ll pay less than everyone else. At Precision Nutrition we like to reward the most interested and motivated people because they always make the best clients. Join the presale list and you’ll save up to 54% off the general public price, which is the lowest price we’ve ever offered.
- You’re more likely to get a spot. To give clients the personal care and attention they deserve, we only open up the program twice a year. Last time we opened registration, we sold out within minutes. By joining the presale list you’ll get the opportunity to register 24 hours before everyone else, increasing your chances of getting in.
If you’re ready to change your body, and your life, with help from the world’s best coaches, this is your chance.
[Note: If your health and fitness are already sorted out, but you’re interested in helping others, check out our Precision Nutrition Level 1 Certification program].
The post Coaching: 35 lessons from Precision Nutrition’s most successful clients. Advice on how to get in your best shape from people who’ve done it. appeared first on Precision Nutrition.
Source: Health1
